
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1607105
Visistor: 1607105 Smoking and related factors in Khmer ethnic people from 25 to 64 years old in Tra Vinh province.
Tabagisme et ses reliés facteurs chez les personnes Khmère de 25 à 64 ans dans la province de Tra Vinh.
B. Nguyen-Thanh1, T. Nguyen-Van1 T. Tran-Thien1, H. Tran-Van2, A. Vo-Thi-Kim3, V. QuangTan4, T. Nguyen-Quynh1, Q. Dinh-Van1, N. Le-Thi1
1: University of Medicine and Pharmacy of Ho Chi Minh City, Vietnam
2: Thang Long University. Hanoi, Vietnam
3: Nam Anh Hospital. Binh Dương, Vietnam
4: Health Department of Binh Duong Province. Vietnam
Corresponding author
Dr. Binh Nguyen-Thanh.
University of Medicine and Pharmacy of Ho Chi Minh City.Vitenam
Email: bsbinh360@gmail.com
ABSTRACT
The present study determined the propotion of smoking and related factors over 1.200 Khmer ethnic people from 25-64 years old at 30 communes and wards in Tra Vinh province, with using random sampling method according to population size.
Results showed that the propotion of smoking was 32.0%. Inside, occasional smoking rate was 3.0%, daily smoking was 29.0%, smoking prevalence among men is higher with 68.0%, was 2.7% in women. Age started is 20.6 ± 5.6 smokers. The smoking habit related to the age, occupation, education, alcohol abuse.
The smoking rate of Khmer people at Tra Vinh was high. The smoking rate had been related to other health behaviors such as alcohol abuse and physical activity.
KEYWORDS: Smoking, Khmer ethnic.
RÉSUMÉ
La présente étude a déterminé la proposition de tabagisme et les facteurs liés à plus de 1.200 ethnies khmers de 25 à 64 ans dans 30 communes et quartiers de la province de Tra Vinh, en utilisant une méthode d'échantillonnage aléatoire selon la taille de la population. Les résultats ont montré que la proposition de fumer était de 32,0%. À l'intérieur, le taux de tabagisme occasionnel était de 3,0%, le tabagisme quotidien était de 29,0%, la prévalence du tabagisme chez les hommes est plus élevée avec 68,0%, était de 2,7% chez les femmes. L'âge commencé est de 20,6 ± 5,6 fumeurs. L'habitude de fumer liée à l'âge, à la profession, à l'éducation, à l'abus d'alcool. Le taux de tabagisme chez les Khmers à Tra Vinh était élevé. Le taux de tabagisme a été lié à d'autres comportements de santé tels que l'abus d'alcool et l'activité physique.
MOTS CLÉS: Tabagisme, Khmère ethnique.
INTRODUCTION
Each year, the global tobacco epidemic kills an estimated 6 million persons in the worldwide, including 600,000 who die from secondhand smoke exposure.
If current trend continues, it is estimated that by 2030, the tobacco use will result in approximately 8 million deaths in the worldwide annually; an estimated 80% of these preventable deaths will occur in low- and middle-income countries [1]. One third to one half of lifetime users die from tobacco products and smokers die an average of 14 years earlier than nonsmokers. Among the estimated one billion smokers in the worldwide, men - women ratio is by four to one. In 14 countries, at least 50% of men smokers, whereas in more than half of these same countries, fewer than 10% of women smokers. If current trend persists, an estimated 500 million persons alive today will die from use of tobacco products. By 2030, tobacco use will result in the deaths of approximately 8 million persons in the worldwide each year [2]. Between 1990 and 2010, the prevalence of tobacco smoking at all ages increased by 1% in men and declined by 2% in women in Iran, but the overall prevalence in the general population was unchanged (12%) [3].
In Vietnam, although the program, policy and public health efforts have been applied to prevent the harms of tobacco products, the smoking rate remains high and the tobacco industry number is still growing. The Global Adult Tobacco Survey (GATS) which conducted in Vietnam in 2010 showed that the smoking rate of Vietnamese male was highest in the world (47.4% of adult men). According to the report of MOH (Ministry of Health) in 2015, the prevalence of smoking in Vietnam was 22.5% of population at the age over 15 years old. Comparison to 2015, the smoking rate was decreased from 23.8% to 22.5%. In which, the smoking rate was reduced from 47.4% to 45.3% in men and from 1.4% to 1.1% in women [4,5]. However, the national reports have not fully aggregated and specified the smoking status in the ethnic minority community who live with different customs, traditional habits and social economic condition. Tra Vinh province has a high density of Khmer minority people who have difficult social economic condition, limited access information and health care service. The risk of smoking and its other related factors could be determined in order to develop the method and policy in protecting and improving public health.
SUBJECTS AND METHODS
Subjects
Khmer minority subjects aged from 25 to 64 years old, living permanent or temporary in the commune over one years were included in the study. The pregnant women or subjects with disability with huchbacks, scoliosis, or foot deformity were excluded.
Methods
Study design
It was a cross-sectional study.
Sample size and selection technique

n: the minimum sample size for each group; p = 0.225 – the ratio of smokers over 15 years old in Vietnam according to the MOH report 2015 [5]; α: the statistic significance level of 0.05 (α=0.05); e = 0.03: resistance tolerance; the design coefficient DE = 2; the ratio of losing sample: 10%; the minimum sample size n = 845 people.
Choosing sample size were 1,200 people.
Choosing sample
Thirty communes were chosen by using random cluster sampling based on population size. There were 40 chosen people each cluster as in population statistics list, which divided into 8 groups of age such as 25-34, 35-44, 45-54, 55-64 years old. Chosen 5 people according to the age groups and gender.
Data collection
Interview was conducted by using structured questionnaire, according to the form of the World Health Organization.
Data analyzing
Data was input and analyzed by medical statistic method using Epi-Data, Stata-12 software. Comparing significant difference in χ² test. The significant threshold was p < 0.05.
Study index
Smoking: smoking any kind of tobacco or quitting smoking < 30 days [6]; smoking frequency: < 10 cigarettes/day, 10-<20 cigarettes/day, and ≥ 20 cigarettes/day; smoking time: < 5 years and ≥ 5 years; lung cancer risk: according to the selection criteria of the American Association for Thoracic Surgery (AATS), smokers ≥ 55 years old and smoked ≥ 30 pack-years (multiplication of packs per day and
years of daily smoking). Alcohol abuse: man: ≥ 5 standard shots (equal 330 ml beer, 30ml brandy or 120ml of wine); woman: ≥ 4 standard shots in anyday in a week. Physical activity: extreme intense activity: ≥ 75 min/ week, average intense activity ≥ 150 min/week or combination of both activity ≥ 600 MET-minute/week.
Study ethics
Benefits and personal information of the object will be protected in accordance with regulations of the
Ethics Council of the National Institute of Hygiene and Epidemiology and Tra Vinh Department of Health.
RESULTS
The ratio of smoking in Khmer minority people from 25-64 years old at Tra Vinh province
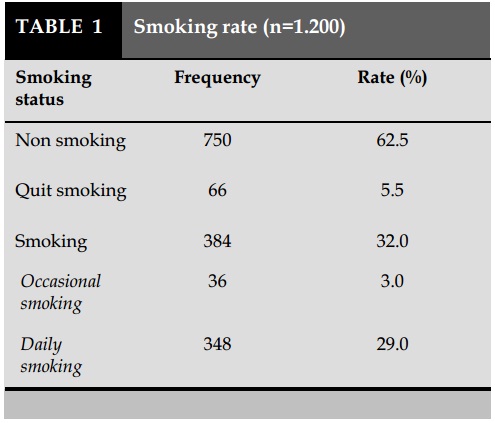
The smoking rate of Khmer people aged 25-64 years at Tra vinh was 32.0%. In which, occasional smoking was 3.0% and daily smoking was 29.0%. The rate of quitting smoking was 5.5% (Table 1).
The smoking time and frequency
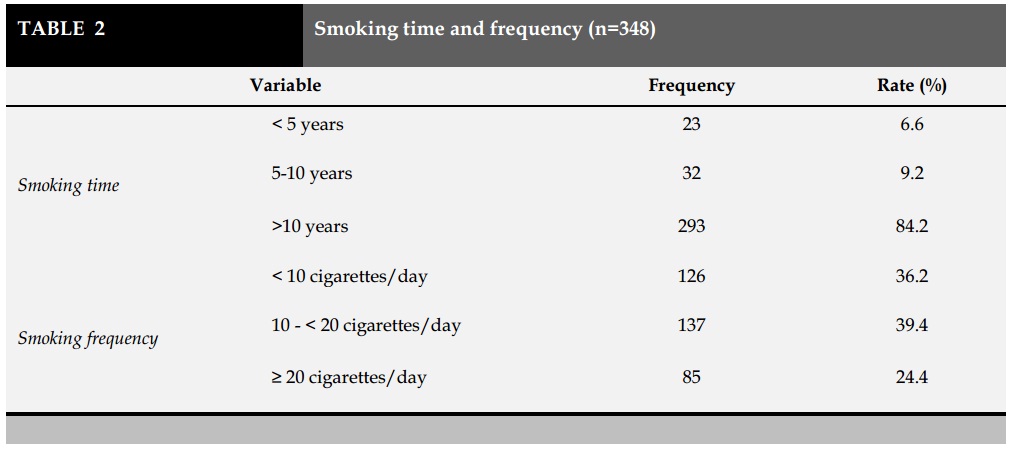
In the daily smoking group, the rate of smoking over 10 years was the highest accounted for 84.2% and the frequency rate of smoking with 10 to 20 cigarettes/ day was 39.4% (Table 2).
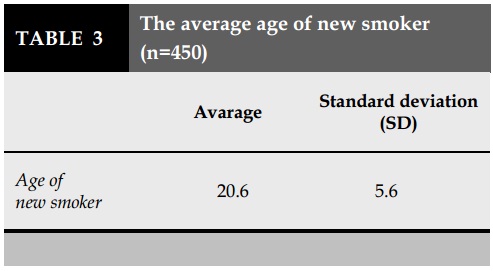
The average age of new smokers
The average age of new smokers who used to smoke or still smoke was 20.6 ± 5.6 years (Table 3).
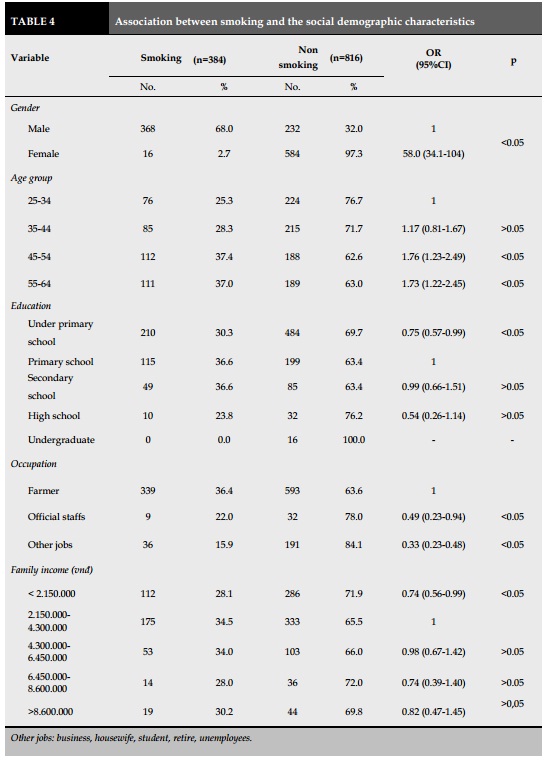
Association of smoking with the social demographic characteristics and behavior (Table 4)
The smoking rate in male was 68.0% while this rate was 2.7% in female (OR=58; p<0.05).
The smoking rate of the age group from 45-54 years old was higher than that in the age group from 25 - 34 years old (OR=1.76 and 1.73, respectively; p<0.05).
The smoking rate of under primary school group was less than the primary school group (OR=0.75, p<0.05). The group of official staffs and other jobs had lower smoking rate than the farmer group (OR=0.49 and 0.33, respectively; p<0.05).
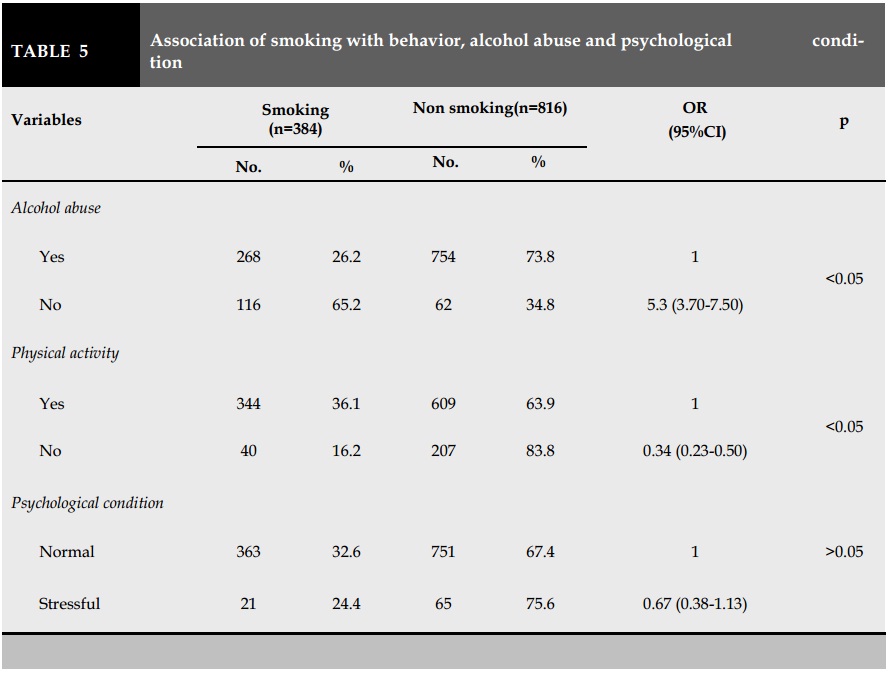
Association of smoking with behavior, alcohol abuse and psychological condition (Table 5)
The smoking rate of the alcohol abuse group was higher than the opposite group (OR=5.3; p<0.05).
The physical activity group had a higher smoking rate than the group of non-physical activity (OR=0.34; p<0.05).
Lung cancer risk (Table 6)
According to the standard criteria of American Association for Thoracic Surgery (AATS), the risk of lung cancer in smokers was about 7.5%.
DISCUSSION
The social demographic characteristics
The percentage of male and female was almost equivalent and also unformly distributed across age groups. The group of having education level under primary school accounted for 57.8% and the farmer was 77.7%. Male and female sex ratio was nearly the same and equally distributed across age groups.
The smoking rate of Khmer people aged 25-64 in Tra Vinh
The result showed that the smoking rate in Khmer people at Tra Vinh was high with 32%, in which 29% were daily smoking (Table 1). Men were major smokers accounted for 68%. The smoking rate in 45-54 and 55-64 years old group were equal at 37% (Table 4). Therefore, the smoking rate in this study was higher than in the report of WHO in 2010 in Vietnam which were 23.8% with 47.4% of male smokers and 29.7% of group aged 45-64 years [4]. The recent report of Vietnam MOH in 2015 pointed out that the smoking rate was 22.5% in adult and 45.3% in male which decreased in comparison with 2010 [5].
The smoking rate in rural area and in ethnic minority people including Khmer people at Tra Vinh was extremely high and remained unchanged. The reasons of this result were included the difficult socioeconomic life, limited knowledge, information access, and health service.
Beside of that, most smokers started to quite smoking early with the average age of starting smoking 20.6 ± 5.6 years old and the rate of smoke exposure time over 10 years was 84.2%. Based on the most
recent data in Vietnam (2010), the prevalence of smoking among adults aged >15 years was 23.8%, with a higher percentage among males (47.4%) than females (1.4%) [7]. Smoker subjects were almost the farmers and the general level of intellectual was limited with the low rate of higher education at secondary and high school. In addition, the difficulties in approaching and changing behavior of the teenagers in this commune. These factors were directly contributed to th reasons of having high percentage of young smokers and the public health problem was affected by the long time of smoking exposure.
The result also pointed out the differences among the smoking rate of the occupation groups. Farmers had higher smoking rate than official staffs and other occupation groups (Table 4). These results could suggest the appropriate and effective interventions and policies for local health managers in the future.
In the present study, the smoking rate of Khmer people in no physical activity group was higher than the group of alcohol independence (OR=0.34; Table 5). Smoking is the leading preventable cause of death among individuals with mental health difficulties (MHD). Cross-sectional analysis of a national representative sample of 8175 community-dwelling adults aged 50 and over from The Irish Longitudinal Study on Ageing (TILDA) was undertaken, smoking and also associated with the presence of smoking-related disease (ORs ranging from 1.24 [1.01-1.51] to 1.62 [1.00-2.62]). These findings underscore the need of attention to the physical health of those with MHD including support for smoking cessation [8].
On the other hand, the smoking rate had been related to other health behaviors such as alcohol abuse and physical activity.
The smoking rate in alcohol abuse group was higher than the group of alcohol independence (OR=5.3;
Table 5). It suggested that the smoking behavior occurred at the same time with other behaviors, especially alcohol abuse. Khmer people have many traditional customs and festivals that why drinking alcohol and smoking were considered as communication in commune.
The risk of lung cancer in Khmer people aged from 25-64 at Tra Vinh
The risk of heart and cancer diseases (especially lung cancer) is higher if having the longer the exposure time with smoke an smoking. According to the American Association for Thoracic Surgery (AATS), people aged ≥55 years old who smoked ≥30 packsyear have a high risk of lung cancer [9]. Despite a reduction in the rate of tobacco smoking, including second-hand smoke, since 1990, smoking exposure remained the fifth leading risk factor for deaths and DALYs in Iran in 2010 [3]. For data in Viet Nam, of the adult respondents, 55.5% believed that smoking may cause lung cancer, stroke, and heart disease [7].
The study of Charafedine et al. [10] provided an estimate of the percentage of cancer in Lebanon by 2018 that has been due to the exposure to risk factors in 2008, lung and laryngeal cancers in both males and females had the largest proportions attributable, with 79% and 72% of lung cancer cases in male and female respectively have been involved to the result of smoking. As for the rest of the cancers associated with smoking, the percentages and relative risks were higher in male than in female. Smoking caused most cancer cases, and it will further add a total of 1800 new cases by 2018. Among many other cancers, lung cancer had the largest proportion attributable of around 75% [10]. This study showed that 7.5% of smokers in Khmer people had the risk of lung cancer in near future (Table 6).
CONCLUSION
The smoking rate of Khmer people at Tra Vinh was high, in which, the daily smoking rate was 29.0%, the smoking rate was 68.0% in male and 2.7% in female. The rate of quitting smoking was very low (5.5%). The average age of smoking was 20.6 ± 5.6. The smoking habit related to the age, occupation, education, alcohol abuse and physical activity.
CONFLIT OF INTEREST
The authors declare that they have no conflit of interest.
REFERENCES
1. Centers of Disease Control and Prevention. Announcement: World No Tobacco Day — May 31, 2017. 2017 [cited 2017; Available from: http:// dx.doi.org/10.15585/mmwr.mm6620a7.
2. Morbidity and Mortality Weekly Report (MMWR), CDC Grand Rounds: Global Tobacco Control. 2014. p. pp.277-280.
3. Ghasemian A, et al., Tobacco Smoking Status and the Contribution to Burden of Diseases in Iran, 1990-2010: findings from the Global Burden of Disease Study 2010. Archives of Iranian Medicine, 2015. 18(8): p. pp.493- 501.
4. WHO, Global Adult Tobacco Survey (GATS) Viet Nam 2010. 2010, Ministry of Health of Viet Nam: Ha Noi.
5. Nam, M.o.H.V., Situation of adult use of cigarettes in Vietnam in 2015, in in Dissemination of the results of the second survey. 2016. 2016: Ha Noi.
6. World, H.O., National Survey for Non-Communicable Disease Risk Factors and Injuries: Using WHO STEPS approach in Timor-Leste - 2014. 2015.
7. D.T. Tran, et al., Tobacco Control in Vietnam. Public health, 2013. 127(2): p. pp.109-118.
8. Burns A, et al., Exploring smoking, mental health and smoking-related disease in a nationally representative sample of older adults in Ireland - A retrospective secondary analysis. Journal of psychosomatic research, 2017. 98: p. pp.78-86.
9. Jaklitsch, M.T. and e. all, The American Association for Thoracic Surgery guidelines for lung cancer screening using low-dose computed tomography scans for lung cancer survivors and other high-risk groups. J Thorac Cardiovasc Surg, 2012. 144(1): p. 33-38.
10. Charafeddine MA, et al., Proportion of cancer in a Middle eastern country attributable to established risk factors. BioMed Central Cancer, 2017. 17(1): p. pp.317-337.

TABLES
REFERENCES
1. Centers of Disease Control and Prevention. Announcement: World No Tobacco Day — May 31, 2017. 2017 [cited 2017; Available from: http:// dx.doi.org/10.15585/mmwr.mm6620a7.
2. Morbidity and Mortality Weekly Report (MMWR), CDC Grand Rounds: Global Tobacco Control. 2014. p. pp.277-280.
3. Ghasemian A, et al., Tobacco Smoking Status and the Contribution to Burden of Diseases in Iran, 1990-2010: findings from the Global Burden of Disease Study 2010. Archives of Iranian Medicine, 2015. 18(8): p. pp.493- 501.
4. WHO, Global Adult Tobacco Survey (GATS) Viet Nam 2010. 2010, Ministry of Health of Viet Nam: Ha Noi.
5. Nam, M.o.H.V., Situation of adult use of cigarettes in Vietnam in 2015, in in Dissemination of the results of the second survey. 2016. 2016: Ha Noi.
6. World, H.O., National Survey for Non-Communicable Disease Risk Factors and Injuries: Using WHO STEPS approach in Timor-Leste - 2014. 2015.
7. D.T. Tran, et al., Tobacco Control in Vietnam. Public health, 2013. 127(2): p. pp.109-118.
8. Burns A, et al., Exploring smoking, mental health and smoking-related disease in a nationally representative sample of older adults in Ireland - A retrospective secondary analysis. Journal of psychosomatic research, 2017. 98: p. pp.78-86.
9. Jaklitsch, M.T. and e. all, The American Association for Thoracic Surgery guidelines for lung cancer screening using low-dose computed tomography scans for lung cancer survivors and other high-risk groups. J Thorac Cardiovasc Surg, 2012. 144(1): p. 33-38.
10. Charafeddine MA, et al., Proportion of cancer in a Middle eastern country attributable to established risk factors. BioMed Central Cancer, 2017. 17(1): p. pp.317-337.
ARTICLE INFO
DOI: 10.12699/jfvp.7.22.2016.sup.1
Conflict of Interest
Non
Date of manuscript receiving
20/7/2016
Date of publication after correction
15/11/2016
Article citation
Nguyen-Thanh B, Nguyen-Van T, Tran-Thien T, Tran-VanH, Vo-Thi-Kim A, QuangTan V, Nguyen-Quynh T, Dinh-Van Q, Le-Thi N. Smoking and related factors in Khmer ethnic people from 25 to 64 years old in Tra Vinh province. J Func Vent Pulm 2016; 22(7): 1-66.



Copyright: jfvpulm.com