
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1735837
Visistor: 1735837Unusual presentation of pulmonary hydatidosis mimicking massive pleural effusion
Présentation inhabituelle de l'hydatidose pulmonaire imitant d’un épanchement pleural massif
H. Haddaoui, K. Bouytse, B. Daher, D. Zagouach, M. Soualhi, J. Bourkadi
Pneumo-Phtisiologie Department, Moulay Youssef Hopital
Faculty of Medicine and Pharmacy of Rabat, Morocco
Corresponding author:
Dr. Hanane Haddaoui. Pneumo-Phtisiologie Department, Moulay Youssef Hopital
Faculty of Medicine and Pharmacy of Rabat, Morocco.
E-mail: hanane.haddaoui@gmail.com
DOI: 10.12699/jfvpulm.12.36.2021.71
Massive pleural effusions are commonly caused by malignancy, parapneumonic effusion, and tuberculosis. Parasitic infections are rare causes of massive pleural effusion.
Echinococcosis or hydatid disease is a major public health problem in poor hygienic environments. The liver and lungs are the most frequently involved organs. Pulmonary disease appears to be more common in younger individuals. Echinococcus multilocularis causes alveolar echinococcosis, which accounts for <5% of all cases of hydatid liver disease and less frequently lung disease.
Here, we present an unusual case of multilocular pulmonary hydatid cysts mimicking massive pleural effusion.
KEYWORDS: Echinococcus multilocularis; Hydatid cyst; Pleural effusion.
Les épanchements pleuraux massifs sont généralement causés par une tumeur maligne, un épanchement parapneumonique et la tuberculose. Les infections parasitaires sont des causes rares d'épanchement pleural massif.
L'échinococcose ou maladie hydatique est un problème majeur de santé publique dans les environnements peu hygiéniques. Le foie et les poumons sont les organes les plus fréquemment touchés. La maladie pulmonaire semble être plus fréquente chez les personnes plus jeunes. Echinococcus multilocularis provoque une échinococcose alvéolaire, qui représente <5% de tous les cas de maladie hépatique hydatique et moins fréquemment de maladie pulmonaire.
Ici, nous présentons un cas inhabituel de kystes hydatiques pulmonaires multiloculaires imitant un épanchement pleural massif.
MOTS CLÉS: Echinococcus multilocularis, kyste hydatique, épanchement pleural
INTRODUCTION
Massive pleural effusion is commonly caused by malignancy and has an incidence of 11.2% 12% of all the pleural effusions. [1] Its etiology and occurrence have remained largely undetermined and therefore not known. Hydatid cyst mimicking as massive effusion is very uncommon.
Here, we report an unusual case of pulmonary hydatid cyst manifested as massive pleural effusion.
CASE REPORT
A 47-years-old male, chronic smoker by 20 packs / year and bricklayer by profession, complained, dry cough, exertion dyspnea, abdominal and right-sided chest pain for the last 3 months. The right-sided chest pain was localized and dull-aching and responded favorably to analgesics. His past medical history was unremarkable for major illness or surgery.
On presentation in general examination, the patient was hemodynamically stable, with a pulse rate of 82 beats/minute, a blood pressure of 120/80 mmHg, and an oral temperature of 37.2 °C. Percussion dullness was noted in the right side of the chest, with normal percussion in the left side. On auscultation, the breathing sounds were found to be decreased in the right side of the chest. Abdominal examination found hepatomegaly.
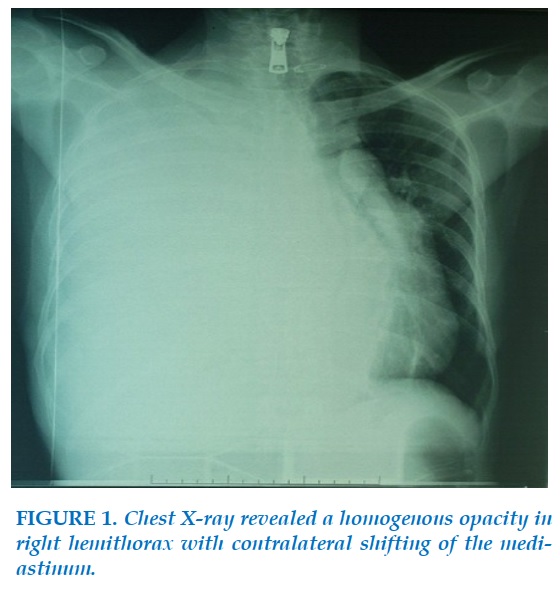
Chest X-ray revealed a homogeneous opacity in the right hemithorax with contralateral shifting of the mediastinum (Figure 1) suggestive of massive pleural effusion.
With medical history of chronic smoking and occupational exposure, differential diagnosis were consisted of malignant metastasis, mesothelium or pleural tuberculosis in our endemic country.
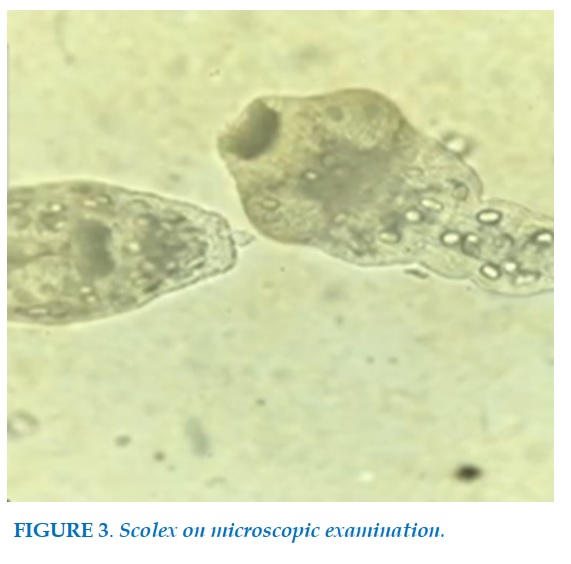
Chest ultrasound was then performed and showed multiple vesicular images (Figure 2). Decision was made to perform an ultrasound-guided thoracocentesis that revealed a clear aspirate which on microscopic examination revealed hooklets of Echinococcus (Figure 3).
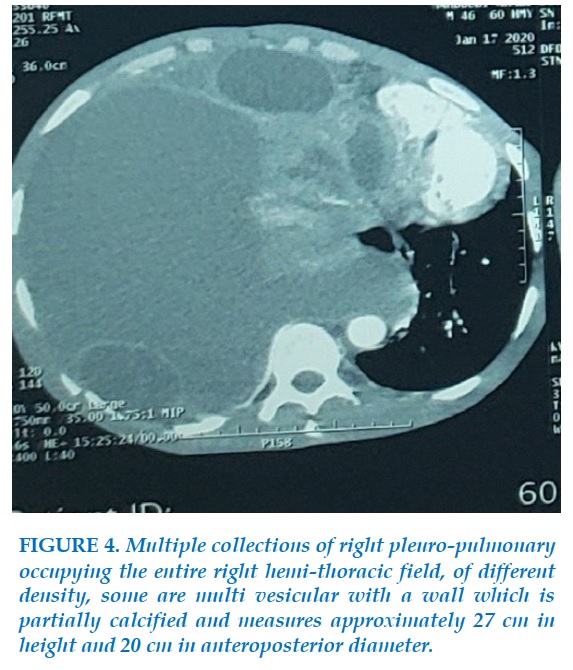
We completed with a chest CT (Figure 4) which showed a significant medial deviation towards the left side with hypotrophy of the left thoracic hemi-field and the presence of multiple collections on the right pleuro-pulmonary space occupying the entire right hemi-thoracic field.
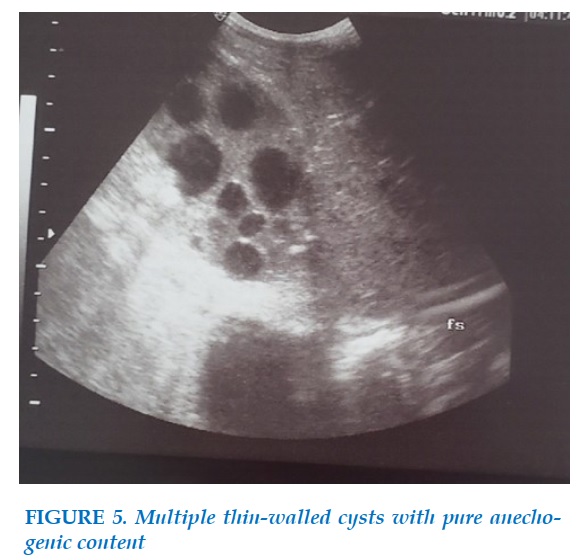
Abdominal ultrasound (Figure 5) showed an enlarged liver, the seat of a voluminous, well-defined formation, occupying the entire heterogeneous right liver containing multiple thin-walled cysts with pure anechogenic content, evoking hydatid cyst classified Grade III in the Gharbi Classification.
Bronchoscopy showed normal endoscopic appearance, no white membrane; research for scolex into bronchial suction fluid was negative.
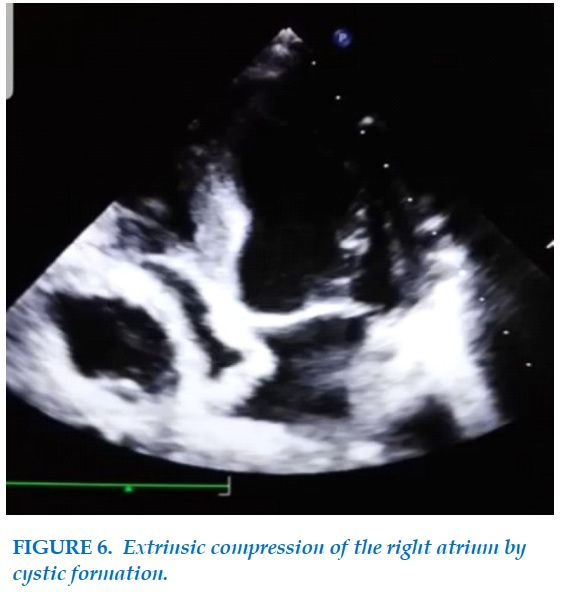
Cardiac ultrasound (Figure 6) revealed extrinsic compression of the right atrium by cystic formation with no impact on cardiac output flow.
A diagnosis of right-sided pleuro-pulmonary multiple hydatid cysts with hepatic location was entertained. The diagnosis was further confirmed by the demonstration of raised serum IgG for Echinococcus. The patient was started on albendazole 15 mg/kg/day twice daily and referred to a cardiothoracic and visceral surgeon for cysts removal.
DISCUSSION
Pleural effusions are a common medical problem with >50 recognized causes, including intra pleural disease or underlying lung, systemic conditions, organ dysfunction, and drugs. Effusions that involve the entire hemithorax or at least two-thirds of it are designated as massive. Massive pleural fluid collection can be caused by a wide range of clinical conditions that can be classified into malignant and non-malignant causes [2]; pleural effusion due to parasitic infection is hence uncommon.
Hydatid disease in humans occurs by infection with the larval stage of the tapeworm Echinococcus granulosus (the dog tapeworm) or Echinococcus multilocularis (the fox tapeworm). Humans acquire the infection by ingesting the eggs due to poor hygiene practices or contaminated food and water [3].
Echinococcus is most commonly reported in pastoral communities of South America, Australia, and the Mediterranean. Morocco is a highly endemic country of EK. The region of the Middle Atlas has been judged to be the area where KS is most widespread by surveys carried out between 2001 and 2004 by Azlaf et al. [4].A total of 23,512 human cases were recorded by the
Ministry of Health of Morocco during the periods 1980-1992 and 2003-2008 [5]. The larvae most often involves the liver (55-70%) followed by the lungs (18-35%); the two organs can be affected simultaneously in about 5-13% of cases [6]. However, any organ may be involved [7]. Echinococcal infestation of the pleura or chest wall has been reported to occur in 0.9-7.4% of patients with hydatid disease [7], [8].
Diagnosis depends mainly on the imaging procedures supported by appropriate serology and often histopathology. CT is probably the best technique to elucidate the nature and location of the cyst to precise their relation with surrounding organs and thus evaluate the cyst preoperatively. Cyst density may serve to differentiate parasitic from nonparasitic cysts [9]. On the basis of density and clinical symptoms, hydatid cysts of the lungs can be classified as simple cysts, complicated cysts, and ruptured cysts (including cysto-bronchial communication). “Inverse crescent” sign as well as “signet ring” sign are commonly recognized as features of pulmonary hydatid cysts on CT. Pathognomonic features in ruptured or complicated hydatid cysts on CT include detached or collapsed endocyst membrane, collapsed daughter cyst membranes, and intact daughter cysts [10]. Though hydatid cysts of the liver commonly undergo calcification, it is rare for pulmonary or mediastinal hydatid cysts to develop calcification.
Magnetic resonance imaging is probably better than CT scanning in the evaluation of postsurgical residual lesions and recurrences [11], [12]. The treatment of choice in the pulmonary hydatid cyst is surgical resection. Although the percutaneous aspiration, injection of cysticidal agent, and Re-aspiration using radiographic guidance (PAIR) method is being routinely used in cases of hydatid liver disease, the WHO currently recommends that PAIR should not be used in case of pulmonary cysts [13]. Surgery should be coupled with albendazole (10–15 mg/kg/day) administration in two doses from 4 days before to at least 1 month after surgery. Anthelminthic therapy before surgery has shown to reduce the risk of recurrence by 3.5 times [14].
CONCLUSION
Pulmonary echinococcosis may rarely present as massive pleural effusion, and this diagnosis can be kept on differential diagnosis in endemic areas. Chest CT is a useful adjunctive diagnostic maneuver and helps in pinning down the underlying etiology.
CONFLICTS OF INTEREST
The authors declare no conflict of interest
REFERENCES
1. Jiménez D, Díaz G, Gil D, Cicero A, Pérez-Rodríguez E, Sueiro A, et al. Etiology and prognostic significance of massive pleural effusions. Respir Med 2005;99:1183-7.
2. Porcel JM, Vives M. Etiology and pleural fluid characteristics of large and massive effusions. Chest 2003;124:978-83.
3. Vlad DC, Neghina AM, Dumitrascu V, Marincu I, Neghina R, Calma CL, et al. Cystic echinococcosis in children and adults: A seven-year comparative study in Western Romania. Foodborne Pathog Dis 2013;10:189-95
4. Azlaf R, Dakkak A. Epidemiological study of the cystic echinococcosis in Morocco. Vet Parasitol. 2006; 137(1-2):83-93.
5. Derfoufi O, Akawa E, Elmaataoui A, Miss E, Esselmani H, Lyagoubi M, et al. Epidemiological profile of cystic echinococcosis in Morocco from 1980 to 2008. Ann Biol Clin. 2012; 70(4):457-61.
6. Arora V, Nijjar IS, Gill KS, Singh G. Case report: Primary hydatid cyst of muscle-a rare site. Ind J Radiol Imaging 2006;16:239-41.
7. Sayir F, Cobanoðlu U, Sehitoðullarý A, Bilici S. Our eight-year surgical experience in patients with pulmonary cyst hydatid. Int J Clin Exp Med 2012;51:64-71.
8. Aribas OK, Kanat F, Gormus N, Turk E. Pleural complications of hydatid disease. J Thorac Cardiovasc Surg 2002;123:492-7.
9. Saksouk FA, Fahl MH, Rizk GK. Computed tomography of pulmonary hydatid disease. J Comput Assist Tomogr 1986;10:226-32.
10. Gouliamos AD, Kalovidouris A, Papailiou J, Vlahos L, Papavasiliou C. CT appearance of pulmonary hydatid disease. Chest 1991;100:1578-81.
11. Koul PA, Koul AN, Wahid A, Mir FA. CT in pulmonary hydatid disease: Unusual appearances. Chest 2000;118:1645-7.
12. Beggs I. The radiology of hydatid disease. AJR Am J Roentgenol 1985;145:639-48.
13. Brunetti E, Kern P, Vuitton DA, Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop 2010;114:1-6.
14. El-On J. Benzimidazole treatment of cystic echinococcosis. Acta Trop 2003;85:243-52.

-FIGURES-

REFERENCES
1. Jiménez D, Díaz G, Gil D, Cicero A, Pérez-Rodríguez E, Sueiro A, et al. Etiology and prognostic significance of massive pleural effusions. Respir Med 2005;99:1183-7.
2. Porcel JM, Vives M. Etiology and pleural fluid characteristics of large and massive effusions. Chest 2003;124:978-83.
3. Vlad DC, Neghina AM, Dumitrascu V, Marincu I, Neghina R, Calma CL, et al. Cystic echinococcosis in children and adults: A seven-year comparative study in Western Romania. Foodborne Pathog Dis 2013;10:189-95
4. Azlaf R, Dakkak A. Epidemiological study of the cystic echinococcosis in Morocco. Vet Parasitol. 2006; 137(1-2):83-93.
5. Derfoufi O, Akawa E, Elmaataoui A, Miss E, Esselmani H, Lyagoubi M, et al. Epidemiological profile of cystic echinococcosis in Morocco from 1980 to 2008. Ann Biol Clin. 2012; 70(4):457-61.
6. Arora V, Nijjar IS, Gill KS, Singh G. Case report: Primary hydatid cyst of muscle-a rare site. Ind J Radiol Imaging 2006;16:239-41.
7. Sayir F, Cobanoðlu U, Sehitoðullarý A, Bilici S. Our eight-year surgical experience in patients with pulmonary cyst hydatid. Int J Clin Exp Med 2012;51:64-71.
8. Aribas OK, Kanat F, Gormus N, Turk E. Pleural complications of hydatid disease. J Thorac Cardiovasc Surg 2002;123:492-7.
9. Saksouk FA, Fahl MH, Rizk GK. Computed tomography of pulmonary hydatid disease. J Comput Assist Tomogr 1986;10:226-32.
10. Gouliamos AD, Kalovidouris A, Papailiou J, Vlahos L, Papavasiliou C. CT appearance of pulmonary hydatid disease. Chest 1991;100:1578-81.
11. Koul PA, Koul AN, Wahid A, Mir FA. CT in pulmonary hydatid disease: Unusual appearances. Chest 2000;118:1645-7.
12. Beggs I. The radiology of hydatid disease. AJR Am J Roentgenol 1985;145:639-48.
13. Brunetti E, Kern P, Vuitton DA, Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop 2010;114:1-6.
14. El-On J. Benzimidazole treatment of cystic echinococcosis. Acta Trop 2003;85:243-52.
ARTICLE INFO
DOI: 10.12699/jfvpulm.12.36.2021.71
Conflict of Interest
Non
Date of manuscript receiving
15/12/2020
Date of publication after correction
15/01/2021
Article citation
Haddaoui H., Bouytse K., Daher B., Zagouach D., Soualhi M., Bourkadi J. Unusual presentation of pulmonary hydatidosis mimicking massive pleural effusion. J Func Vent Pulm 2021;36(12):71-74



Copyright: jfvpulm.com