
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1717167
Visistor: 1717167 Pulmonary tuberculoma associated with multifocal osteoarticular tuberculosis
Tuberculome pulmonaire associé à une tuberculose multifocale ostéoarticulaire
R. Bouchentouf1,2
1 : Lung disease service, Avicenna Military Hospital, Marrakech. Morocco
2 : PCIM laboratory, Caddi Ayyad University, Marrakech. Morocco
Corresponding author
Dr Bouchentouf Rachid
Lung Disease Department. Avicenna Military Hospital. 12 Bd la résistance. Marrakech 40000. Morocco.
E-mail: bouchentouf_rachid@yahoo.f
ABSTRACT
Introduction. Tuberculosis (TB) remains a global public health burden, is a major cause of morbidity and mortality. TB involves both pulmonary and extra pulmonary sites.
Observation. We report the case of a 27 year-old woman who presents sacroiliitis and coxarthritis tuberculosis with pulmonary involvement. The symptoms were insidious and no specific and mimic malignancy disease. Radiological features particularly CT pelvis scan showed osteoarticular lesions in right sacroiliac joint and left coxemoral joint.
The diagnosis was established by histology from both synovial tissue and lung biopsy specimens. The outcome was favorable following adapted antitberculosis treatment.
Conclusion. Sometimes the presentation of tuberculosis is atypical such the association between lung nodule and osteoaricular when the diagnosis and the treatment are a challenge.
KEYWORDS: Multifocal osteoarticular tuberculosis; Pulmonary tuberculoma; Immunocompetent
RÉSUMÉ
Introduction. La tuberculose reste un fardeau mondial pour la santé publique et une cause majeure de morbidité et de mortalité. La tuberculose concerne à la fois les sites pulmonaires et extra pulmonaires.
Observation. Nous rapportons le cas d'une femme de 27 ans présentant une sacroiliite et une coxarthrite tuberculeuse avec atteinte pulmonaire. Les symptômes étaient insidieux et aucune maladie maligne spécifique et mimique. Les caracté-ristiques radiologiques, en particulier la tomodensitométrie du bassin, ont révélé des lésions ostéoarticulaires dans l'articulation sacro-iliaque droite et l'articulation coxémorale gauche.
Le diagnostic a été établi par histologie à partir d'échantillons de biopsie de tissu synovial et de poumon. L'évolution était favorable après un traitement antitberculeux adapté.
Conclusion. Parfois, la présentation de la tuberculose est atypique, par exemple l'association entre le nodule pulmonaire et l'ostéo-aniculaire lorsque le diagnostic et le traitement posent problème.
MOTS CLÉS: Tuberculose ostéoarticulaire multifocale; tuberculome pulmonaire, immunocompétent
INTRODUCTION
Tuberculosis (TB) remains a global public health burden, is a major cause of morbidity and mortality despite universal availability of effective chemotherapy. According of the world Health Organization (WHO), approximately 10 million new case of TB occur every year worldwide [1]. The pulmonary tuberculoma is a well circumscribed nodule or mass in the lungs, caused by Mycobacterium tuberculosis. It is encapsulated by multiple concentric layers of connective tissue. It is a rare pulmonary tuberculosis presentation, and the one of the most common benign pulmonary nodules. It represents 5-24% of resected solitary pulmonary nodules and its size varies from 1 to 10 cm in diameter [2].
Skeletal TB represents 2 to 5% of TB cases in general, and 11 to 15% of extra pulmonary tuberculosis. [3]When tubercular osteo-articular lesions occur simultaneously at two or more locations in the skeletal system are termed multifocal skeletal tuberculosis [4]. It’s uncommon entity even in endemic countries like Morocco. Non specific clinical manifestation and radiological findings mimic neoplasic disease especially with it was associated with pulmonary nodule.
We present a case of tuberculosis osteoarticular multifocal tuberculosis (sacroiliitis and coxitis) with pulmonary tuberculoma in immunocompetent patient in which the diagnosis and treatment of which was a challenge.
OBSERVATION
27 year-old woman with the lower socio-economic status, vaccine with BCG, without previous trauma, was complaining about recurrent right buttock back pain since 11 months in a context of impaired general condition.
The clinical examination revealed a pelvic asymmetry with unequal leg, a painless mass over the lateral aspect of her right hip. The usual blood tests showed normocytic normochromic anemia with a 10 g/dl Hb, normal leukocyte count, a 35 mg/l CRP.
Renal and hepatic biological assessments were normal. The tuberculin skin test was positive at 10 mm and HIV status was negative.
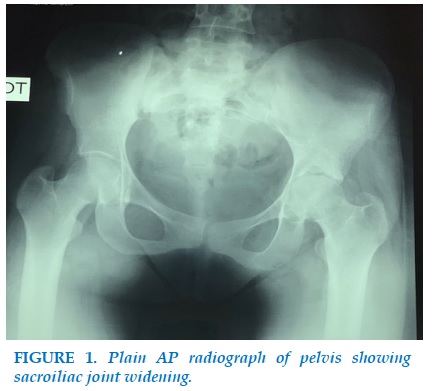
Pelvis radiographs showed a narrowing coxofemoral joint space with demineralization and geodes of the left femoral head (Figure 1).
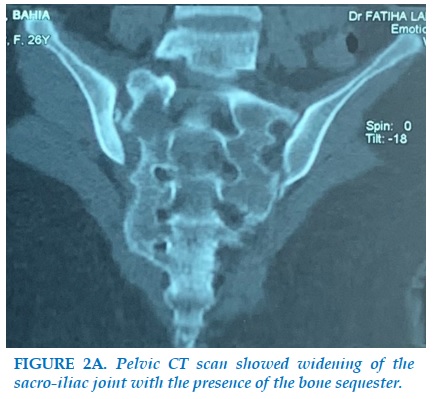
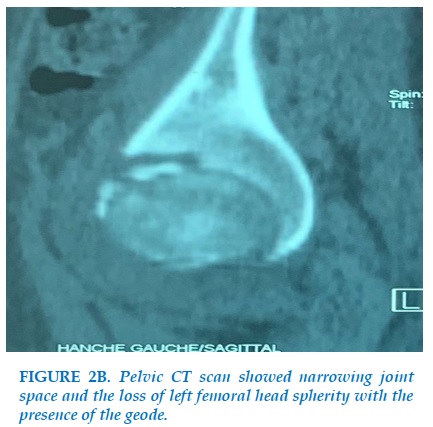
Pelvic CT scan showed an asymmetric basin, widening of the sacro-iliac joint with the presence of the bone sequester (Figure 2 a), and a narrowing joint space and the loss of left femoral head spherity with the presence of the geode (Figure 2 b).
The search for germs in the joint fluid was negative on direct examination and the histological study of the synovial performed after a CT guided biopsy showed an epitheloid giant cell granuloma with caseous necrosis suggestive of osteoarticular tuberculosis.
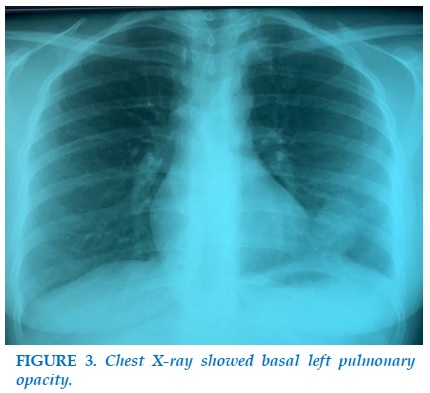
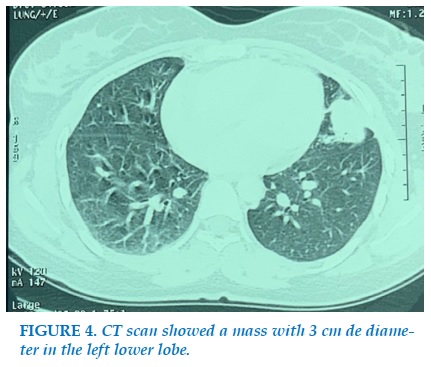
Chest X-ray showed basal left pulmonary opacity (Figure 3). CT scan showed a mass with 3 cm de diameter in the left lower lobe without mediastinal adenopathies (Figure 4).
The bronchoscopy showed inflammation 1ST degree in the left lower lobe. Koch bacillus research in sputum was negative on direct examination.
The histological study of the lung performed after a CT guided biopsy showed confirmed the diagnosis of tuberculosis. The patient received antituberculous regimen with rifampicin, isoniazid and ethambutol for 2 months, then isoniazid and rifampicin combination for 7 months with good clinical and radiological evolution.
DISCUSSION
Pulmonary tuberculoma is a rare entity, even in immunocompetent adults; it develops in 6-9% of the post-primary TB patients [5].
Multifocal osteoarticular tuberculosis is an uncommon entity; it’s associated more with an immunedepression like HIV (Human Immunodeficiency Virus) infection.
Joint involvement may be secondary to direct invasion from an adjacent focus of TB osteomyelitis or even may result from hematogenous dissemination.
The lung is the primary focus in 75% of cases [6].
The association tuberculoma and multifocal osteoarticular tuberculosis is rarely reported. General symptoms are inconstant, usually of moderate importance, and combine variably asthenia, anorexia, weight loss, night sweats and low-grade fever.
The blood tests such as ESR and CRP have little diagnostic value. The skin tuberculin test or IGRA (Interferon gamma releasing assay) tests are of little interest.
CT scan of the chest and the pelvis has shown several advantages over conventional radiology in early diagnosis and follow-up of TB. Pulmonary tuberculoma is difficult to differentiate from primary or metastatic lung cancer.
The use of contrast-enhanced dynamic CT parameters in the diagnosis of active pulmonary tuberculoma the specificity was 96.4% and sensitivity was 77.1%. Subjects with active tuberculomas had significantly higher peak height values than inactive ones [7].
CT of the pelvis or MRI are more helpful for early detection of osteoarticular tuberculosis. CT scan shows clearly the extent of joint destruction and MRI delineates the abscess in the soft tissues. MRI may also contribute to the differential diagnosis from a soft tissue tumor or pyogenic arthritis [8].
The diagnosis of pulmonary tuberculoma and osteoarticular tuberculosis remains a challenge because it usually requires an invasive procedure such as percutaneous needle aspiration or open biopsy.Extrapulmonary locations of mycobacterium and tuberculoma are paucibacillary and culture remains the reference method in the diagnosis and determination of antibiotic susceptibility of isolates.
Hisopathological diagnosis can be confirmed by presence of caseation necrosis, epithelioid cell granuloma and Langerhans giant cells.
Pulmonary tuberculoma respond poorly to antituberculosis treatment and often requires long-term treatment. In Morocco osteoarticular tuberculosis should be treated with rifampicin, isoniazid and ethambutol for two months, followed by rifampicin and isoniazid for 7 more months.
The response to medical treatment alone in tuberculoma is strongly related to its size and its number; sometimes the combination of surgery with medical treatment will be the best approach [9].
In our case the outcome was favorable only with medical treatment
CONCLUSION
Multifocal osteoarticular tuberculosis and pulmonary tuberculoma are rare immunocompetent patient .The radiological end clinical features are non specific and can mimic neoplasic disease. Early diagnosis and well conducted treatment improves the prognosis.
CONFLICT OF INTEREST
None
REFERENCES
1. WHO global tuberculosis report 2018. https://www.who.int/tb/ publications /global report.
2. Delgado-Pecellín I, Molinos-Quintana A, ObandoSantaella I. Giant pulmonary tuberculoma: atypical form of presentation of primary tuberculosis in childhood. Arch Bronconeumol 2011; 47: 55-6.
3. Babhulkar SS. Unusual manifestations of osteoarticular tuberculosis. Clin Orthop Relat Res 2002; 398:114-20.
4. Amin MU, Shafique M, Mahmood R, Ali L, Nadeem A. Multocal osseous tuberculosis involving hands and feet . J College Physic Surg Pakistan 2008; 18:244-245.
5. Andreu J, Cáceres J, Pallisa E, et al. Radiological man ifestations of pulmonary tuberculosis. Eur J Radiol 2004;51:139-49.
6. Indumathi CK, Vikram Kumar S, Lewin S, Prasanna Kumar K. Multifocal skeletal tuberculosis .Pediatric infectious Disease 2010,7:45-47.
7. Tateishi U, Kusumoto M, Akiyama Y, et al. Role of contrast-enhanced dynamic CT in the diagnosis of active tuberculoma. Chest 2002;122:1280-4.
8. Hong SH, Kim SM, Ahn JM, Chung HW, Shin MJ, Kang HS (2001) Tuberculous versus pyogenic arthritis: MR imaging evaluation. Radiology 2001; 218 (3):848-853.
9. Souilamas R, Riquet M, Barthes FP, et al. Surgical treatment of active and sequelar forms of pulmonary tuberculosis. Ann Thorac Surg 2001;73: 443-7.

FIGURES
REFERENCES
1. WHO global tuberculosis report 2018. https://www.who.int/tb/ publications /global report.
2. Delgado-Pecellín I, Molinos-Quintana A, ObandoSantaella I. Giant pulmonary tuberculoma: atypical form of presentation of primary tuberculosis in childhood. Arch Bronconeumol 2011; 47: 55-6.
3. Babhulkar SS. Unusual manifestations of osteoarticular tuberculosis. Clin Orthop Relat Res 2002; 398:114-20.
4. Amin MU, Shafique M, Mahmood R, Ali L, Nadeem A. Multocal osseous tuberculosis involving hands and feet . J College Physic Surg Pakistan 2008; 18:244-245.
5. Andreu J, Cáceres J, Pallisa E, et al. Radiological man ifestations of pulmonary tuberculosis. Eur J Radiol 2004;51:139-49.
6. Indumathi CK, Vikram Kumar S, Lewin S, Prasanna Kumar K. Multifocal skeletal tuberculosis .Pediatric infectious Disease 2010,7:45-47.
7. Tateishi U, Kusumoto M, Akiyama Y, et al. Role of contrast-enhanced dynamic CT in the diagnosis of active tuberculoma. Chest 2002;122:1280-4.
8. Hong SH, Kim SM, Ahn JM, Chung HW, Shin MJ, Kang HS (2001) Tuberculous versus pyogenic arthritis: MR imaging evaluation. Radiology 2001; 218 (3):848-853.
9. Souilamas R, Riquet M, Barthes FP, et al. Surgical treatment of active and sequelar forms of pulmonary tuberculosis. Ann Thorac Surg 2001;73: 443-7.
ARTICLE INFO
DOI: 10.12699/jfvpulm.10.30.2020.59
Conflict of Interest
Non
Date of manuscript receiving
12/12/2019
Date of publication after correction
15/02/2020
Article citation
Bouchentouf R. Pulmonary tuberculoma associated with multifocal osteoarticular tuberculosis. J Func Vent Pulm 2020;33(11):59-62



Copyright: jfvpulm.com