
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1750079
Visistor: 1750079Summarized Vietnamese Guidelines for Diagnosis and Treatment of Adults with Obstructive Sleep Apnea
Résumé des Recommandations Vietnamiennes de Diagnostique et Traitement des Apnées du Sommeil chez les Adultes
Sy Duong-Quy, Hoang Nguyen-Huu, Quan Vu-Tran-Thien, Khue Bui-Diem, Giap Vu-Van, Tien Hoang-Anh, Sang Nguyen-Minh, Hanh Nguyen-Hieu, Thu Nguyen-Ngoc-Phuong, Si Tran-Duc, Tinh Vo-Van, Minh Hoang, Thai Nguyen-Duy, Thuy Phan-Thanh, Thanh Nguyen-Ngo-Hai, Linh Tran-Thanh-Duy, Lien Nguyen-Thi-Hong, Quynh Tran-Xuan, Nhi Nguyen-Thi-Y, Thu Vo-Pham-Minh, Tram Tang-Thi-Thao, Anh Nguyen-Tuan, Toi Nguyen-Van, Ha Ngo-Duy-Tuy, Linh Pham-Van, Huyen Nguyen-Xuan-Bich, Duc Nguyen-Hong, Huong Le-Thi-Minh, Thuy Tran-Phan-Chung, Vinh Nguyen-Nhu, Bao Le-Khac*
Steering Committee of Obstructive Sleep Apnea Guidelines Vietnam Society of Sleep Medicine—VSSM. Vietnam
Corresponding author:
Pr. Sy DUONG-QUY, MD, PhD, FCCP. President of Vietnam Society of Sleep Medicine
Email: sduongquy.jfvp@gmail.com
ABSTRACT
The prevalence of OSA in adults over 18 years old has been reported to be 8.5% in this country (EPSASIE study). OSA with symptoms of daytime sleepiness contributes to patient fatigue, reduced cognitive activity, work performance and quality of life. Excessive daytime sleepiness causes decreased attention and concentration, which is the cause of traffic and occupational accidents.
OSA also increases the incidence of metabolic syndrome and diabetes and the risk of non-alcoholic fatty liver disease. OSA is a common disease, causing a lot of burden on health, medical care and socio-economics. It is necessary to screen patients with OSA at the primary health care for early diagnosis and timely treatment, helping to avoid harmful consequences of the disease. Diagnosis of OSA is based on polysomnography or polysomnography.
Treatment is based on the cause and severity of the disease and aims to improve symptoms. Medical treatment for OSA includes behavioral changes and sleep hygiene, position therapy, non-invasive mechanical ventilation with CPAP (continuous positive airway pressure) or use of mandibular advancement device, associated with physical therapy.
KEYWORDS: Guidelines; Obstructive sleep apnea; Prevalence; Sleepiness; OSA; CPAP .
RÉSUMÉ
La prévalence de l'AOS chez les adultes de plus de 18 ans serait de 8,5 % dans ce pays (étude d’EPSASIE). L'AOS accompagnée de symptômes de somnolence diurne contribue à la fatigue des patients, à une réduction de l'activité cognitive, des performances au travail et de la qualité de vie. Une somnolence diurne excessive entraîne une diminution de l’attention et de la concentration, ce qui est à l’origine d’accidents de la route et du travail.
L'AOS augmente également l'incidence du syndrome métabolique et du diabète ainsi que le risque de stéatose hépatique non alcoolique. L’AOS est une maladie courante qui pose un lourd problème sur la santé, les soins médicaux et la situation socio-économique. Il est nécessaire de dépister les patients atteints d'AOS dans les soins de santé primaires pour un diagnostic précoce et un traitement rapide, contribuant ainsi à éviter les conséquences néfastes de la maladie. Le diagnostic de l'AOS repose sur la polysomnographie ou la polysomnographie.
Le traitement est basé sur la cause et la gravité de la maladie et vise à améliorer les symptômes. Le traitement médical de l'AOS comprend des changements de comportement et d'hygiène du sommeil, une thérapie de position, une ventilation mécanique non invasive avec PPC (pression positive continue des voies respiratoires) ou l'utilisation d'un dispositif d'avancement mandibulaire, associé à une thérapie physique.
MOTS CLÉS: Recommandations; Apnées obstructive du sommeil; Prévalence; Somnolence; AOS; PPC.
PREVALENCE AND BURDEN OF OSA
Obstructive sleep apnea (OSA) is a common medical condition, with an average frequency of 22% (range 9-37%) in men and 17% (range 4-50%) in women. gender [1]. It has been estimated that there are more than 900 million people have OSA [2-5]. However, OSA remains underconcerned because 93% of women and 82% of men with moderate to severe OSA remain undiagnosed [6]. According to estimates, in Vietnam there are more than 4 million adults over 30 years old with OSA and among them, about 2 million people have moderate-severe OSA [4]. The prevalence of OSA in adults over 18 years old is reported to be 8.5% in this country [5]. OSA with symptoms of daytime sleepiness contributes to patient fatigue, reduced cognitive activity, work performance and quality of life. Excessive daytime sleepiness causes decreased attention and concentration, which is the cause of traffic and occupational accidents [7]. In 2000, in the US, more than 800,000 drivers were recorded in car crashes related to OSA, causing nearly 16 billion USD in damages and 1,400 deaths [8].
OSA is characterized by collapse of the upper airway during sleep leading to partial or complete disruption of airflow to the lungs resulting in respiratory events including apnea and/or hypopnea and may be associated with associated with decreased blood oxygen saturation, hypercapnia and/or microarousals and sleep fragmentation [9]. OSA is a risk factor for chronic diseases such as hypertension, pulmonary hypertension, coronary artery disease, heart failure, and stroke. OSA also increases the incidence of metabolic syndrome and diabetes [10-15] and the risk of non-alcoholic fatty liver disease which is one of the common causes of cirrhosis [16]. The rate of mental disorders increases significantly in subjects with OSA. Previous study showed that over 110,000 subjects with OSA, there was a significant increase in mental disorders including 21.8% depression, 16.7% anxiety, 11.9% had post-traumatic disorder, 5.1% had psychosis, and 3.3% had bipolar disorder [17].
SCREENING FOR OSA IN THE COMMUNITY
Key message
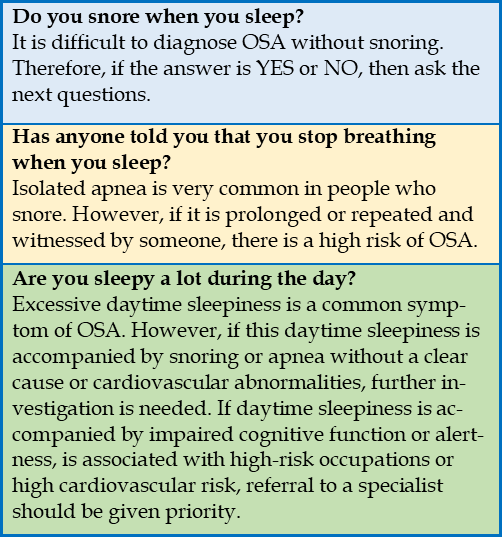
Screening tool
Medical staff can use the following 3 simple questions to screen for OSA in all patients coming to the primary care for any reason, thereby considering further investigation of medical history and related symptoms as needed (Table 1).
TABLE 1. Three questions to screen patients suspected of having sleep apnea.
DIAGNOSIS OF OSA IN ADULTS
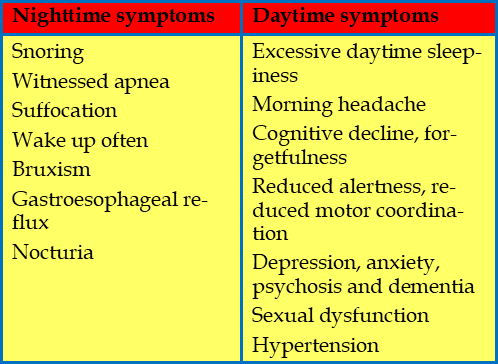
Symptoms of OSA in adults are included in Table 2 [18].
TABLE 2. Nighttime and daytime symptoms of OSA.
Diagnosis of OSA is based on polysomnography. The recommendations of the American Academy of Sleep Medicine (AASM) for the diagnosis of obstructive sleep apnea (OSA) [19] can be applied in Vietnam:
Note:
*Uncomplicated patients: no central sleep apnea, hypoventilation and hypoxia, cardiovascular or respiratory disease, respiratory muscle weakness, history of stroke, chronic opioid use , excessive central sleepiness, sleepwalking, sleep-related movement disorders, severe insomnia; ** High risk of moderate-high OSA: excessive daytime sleepiness + 2/3 criteria: frequent loud snoring, episodes of apnea or gasping or choking, or a diagnosis of hypertension; ***Clinically appropriate: no conditions identified by a physician as likely to interfere for successful diagnosis and treatment using SN-PSG.
OSA is diagnosed according to the criteria of ICSD (International Classification of Sleep Disorders), version 3, 2014 as followed [20]:
-ders, cognitive disorders, hypertension, coronary artery disease, stroke, congestive heart failure, atrial fibrillation or type 2 diabetes.
Or
Classification of OSA severity in adults is defined as following [20]:
15 >Apnea-Hypopnea Index (AHI) ≥5.
30 >Apnea-Hypopnea Index (AHI) ≥15.
Apnea-Hypopnea Index (AHI) ≥30.
TREATMENT OF OSA IN ADULTS
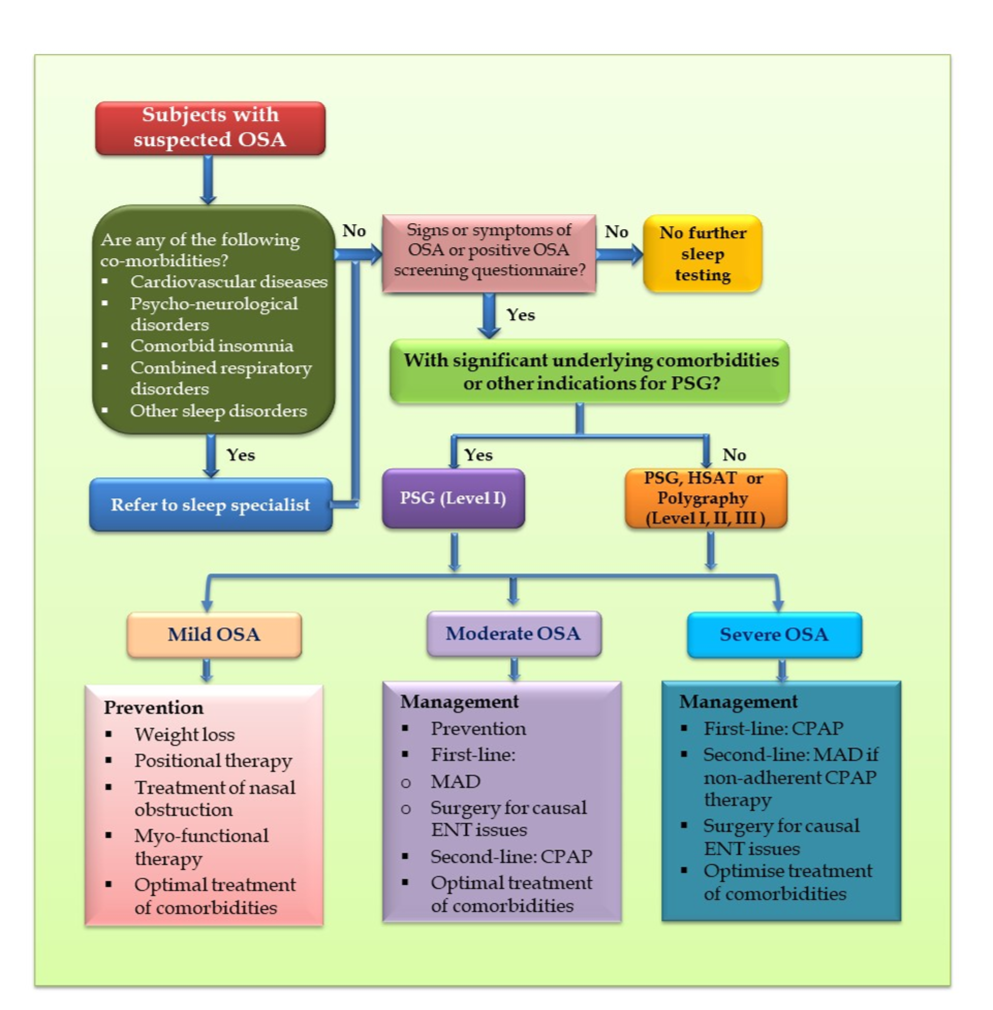
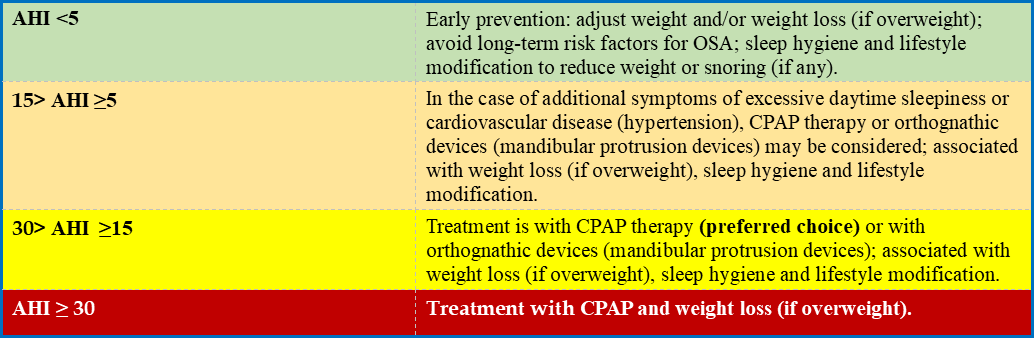
The choice of treatment methods for adults with OSA in Vietnam (or other emergent countries) can be based on the AHI index (Table 3 and Figure 1).
FIGURE 1. Algorithm for diagnosis and treatment of OSA.
CPAP: continuous positive airway pressure; HSAT: home sleep apnea testing; MAD: mandibular advancement device; OSA: obstructive sleep apnoea; PSG: polysomnography.
TABLE 3. Prevention and treatment options based on AHI index [24-26].
PERSONALIZED DIAGNOSIS AND TREATMENT FOR ADULTS WITH OSA
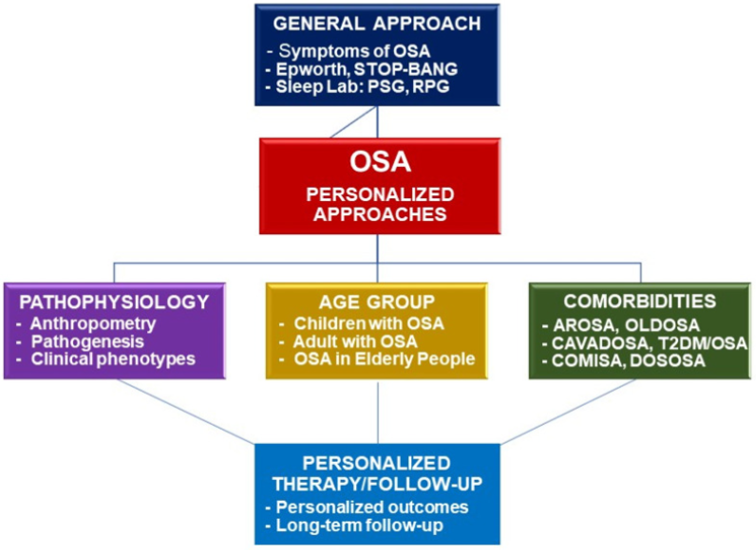
The needs of personalized approaches for subjects with OSA in Vietnam and other emerging countries (Figure 2).
This is due to differences in people morphology, diversity in clinical phenotypes, and different resources in diagnosis and treatment of OSA in adults [27]. Therefore, a personalized medicine approach to diagnosis and treatment of OSA is necessary for physicians in clinical practice (Figure 2).
Adults without serious underlying medical conditions, polysomnography at sleep labs may be an inappropriate and inconvenient testing modality compared to home sleep apnea testing (HSAT).
In addition, the apnea–hypopnea index should not be considered as a single parameter for making treatment decisions [27]. The treatment of OSA should be personalized and based on individual tolerance to sleep-quality-related parameters measured by the microarousal index, harmful effects of OSA on the cardiovascular system related to severe hypoxia, and patients’ comorbidities.
The current treatment options for OSA include sleep hygiene, weight loss, lifestyle modification, position therapy, CPAP therapy, oral appliance, surgery, and other alternative treatments has been recommended for emerging countries [26-28]. Although CPAP therapy has been recommended as a cornerstone treatment for moderate-to-severe OSA in adults, not all patients can afford or tolerate CPAP therapy in these countries.
FIGURE 2. Framework of personalized approaches for diagnosis and treatment of OSA (26).
OSA: obstructive sleep apnea; PSG: polysomnography; RPG: respiratory polygraphy; AROSA: allergic rhinitis and OSA; OLDOSA: obstructive lung disease and OSA; CAVADOSA: cardiovascular diseases and OSA; T2DM: type 2 diabetes mellitus; COMISA: comorbid insomnia and OSA; DOSOSA: Down syndrome and OSA.
CONFLIT OF INTERESTS
The authors declare no conflit of interest.
REFERENCES
| 1. Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. Journal of thoracic disease. 2015;7(8):1311-22. |
| 2. Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, et al. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017;34:70-81. |
| 3. Jessie P. Bakker AM, Sanjay R. Patel. Obstructive Sleep Apnea: Epidemiology of Sleep Apnea. In: Badr MS, editor. Essentials of Sleep Medicine: Humara Press; 2012. p. 95 - 100. |
| 4. Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-98. |
| 5. Duong-Quy S, Dang Thi Mai K, Tran Van N, Nguyen Xuan Bich H, Hua-Huy T, Chalumeau F, Dinh-Xuan AT, Soyez F, Martin F. Study about the prevalence of the obstructive sleep apnoea syndrome in Vietnam. Rev Mal Respir. 2018 Jan;35(1):14-24. |
| 6. Pang KP, Terris DJ. Screening for obstructive sleep apnea: an evidence-based analysis. Am J Otolaryngol. 2006;27(2):112-8. |
| 7. Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirology. 2020;25(7):690-702. |
| 8. Sassani A, Findley LJ, Kryger M, Goldlust E, George C, Davidson TM. Reducing motor-vehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Sleep. 2004;27(3):453-8. |
| 9. Dempsey JA, Veasey SC, Morgan BJ, O'Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47-112. |
| 10. Bouzerda A. Cardiovascular risk and obstructive sleep apnea. Pan Afr Med J. 2018;29:47. |
| 11. Zhai AB, Yip A, Haddad H. Heart failure and sleep-disordered breathing. Curr Opin Cardiol. 2016;31:224-8. |
| 12. Lyons OD, Ryan CM. Sleep Apnea and Stroke. Can J Cardiol. 2015;31(7):918-27. |
| 13. Perez-Carbonell L, Bashir S. Narrative review of sleep and stroke. J Thorac Dis. 2020;12(Suppl 2):S176-S90. |
| 14. Reutrakul S, Mokhlesi B. Obstructive Sleep Apnea and Diabetes: A State of the Art Review. Chest. 2017;152(5):1070-86. |
| 15. Fallahi A, Jamil DI, Karimi EB, Baghi V, Gheshlagh RG. Prevalence of obstructive sleep apnea in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab Syndr. 2019;13(4):2463-8. |
| 16. Turkay C, Ozol D, Kasapoglu B, Kirbas I, Yildirim Z, Yigitoglu R. Influence of obstructive sleep apnea on fatty liver disease: role of chronic intermittent hypoxia. Respiratory care. 2012;57(2):244-9. |
| 17. Sharafkhaneh A, Giray N, Richardson P, Young T, Hirshkowitz M. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep. 2005;28(11):1405-11. |
| 18. Leh-Kiong H CG. Signs and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance. 2020:6-12. |
| 19. Kapur VK, Auckley DH, Chowdhuri S, Kuhlmann DC, Mehra R, Ramar K, et al. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3):479-504. |
| 20. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387-94. |
| 21. Araghi MH, Chen YF, Jagielski A, Choudhury S, Banerjee D, Hussain S, et al. Effectiveness of lifestyle interventions on obstructive sleep apnea (OSA): systematic review and meta-analysis. Sleep. 2013;36(10):1553-62, 62a-62e. |
| 22. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. The Cochrane database of systematic reviews. 2006(1):Cd001106. |
| 23. Schwab RJ, Badr SM, Epstein LJ, Gay PC, Gozal D, Kohler M, et al. An official American Thoracic Society statement: continuous positive airway pressure adherence tracking systems. The optimal monitoring strategies and outcome measures in adults. American journal of respiratory and critical care medicine. 2013;188(5):613-20. |
| 24. Epstein LJ, Kristo D, Strollo PJ, Jr., Friedman N, Malhotra A, Patil SP, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2009;5(3):263-76. |
| 25. Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2019 Feb 15;15(2):335-343. |
| 26. Jacobowitz O, Afifi L, Penzel T, Poyares D, Marklund M, Kushida C; Governing Council of the World Sleep Society. Endorsement of: "treatment of adult obstructive sleep apnea with positive airway pressure: an American academy of Sleep Medicine Clinical Practice Guideline" by World Sleep Society. Sleep Med. 2022 Jan;89:19-22. |
| 27. Duong-Quy S, Nguyen-Huu H, Hoang-Chau-Bao D, Tran-Duc S, Nguyen-Thi-Hong L, Nguyen-Duy T, Tang-Thi-Thao T, Phan C, Bui-Diem K, Vu-Tran-Thien Q, Nguyen-Ngoc-Phuong T, Nguyen-Nhu V, Le-Thi-Minh H, Craig T. Personalized Medicine and Obstructive Sleep Apnea. J Pers Med. 2022 Dec 8;12(12):2034. |
| 28. BaHammam AS, Han F, Gupta R, Duong-Quy S, Al-Abri MA, Jahrami HA, Song P, Desudchit T, Xu L, Hong SB. Asian accreditation of sleep medicine physicians and technologists: practice guidelines by the Asian Society of Sleep Medicine. Sleep Med. 2021 May;81:246-252. |

Figures - Tables
REFERENCES
| 1. Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. Journal of thoracic disease. 2015;7(8):1311-22. |
| 2. Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, et al. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017;34:70-81. |
| 3. Jessie P. Bakker AM, Sanjay R. Patel. Obstructive Sleep Apnea: Epidemiology of Sleep Apnea. In: Badr MS, editor. Essentials of Sleep Medicine: Humara Press; 2012. p. 95 - 100. |
| 4. Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-98. |
| 5. Duong-Quy S, Dang Thi Mai K, Tran Van N, Nguyen Xuan Bich H, Hua-Huy T, Chalumeau F, Dinh-Xuan AT, Soyez F, Martin F. Study about the prevalence of the obstructive sleep apnoea syndrome in Vietnam. Rev Mal Respir. 2018 Jan;35(1):14-24. |
| 6. Pang KP, Terris DJ. Screening for obstructive sleep apnea: an evidence-based analysis. Am J Otolaryngol. 2006;27(2):112-8. |
| 7. Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirology. 2020;25(7):690-702. |
| 8. Sassani A, Findley LJ, Kryger M, Goldlust E, George C, Davidson TM. Reducing motor-vehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Sleep. 2004;27(3):453-8. |
| 9. Dempsey JA, Veasey SC, Morgan BJ, O'Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47-112. |
| 10. Bouzerda A. Cardiovascular risk and obstructive sleep apnea. Pan Afr Med J. 2018;29:47. |
| 11. Zhai AB, Yip A, Haddad H. Heart failure and sleep-disordered breathing. Curr Opin Cardiol. 2016;31:224-8. |
| 12. Lyons OD, Ryan CM. Sleep Apnea and Stroke. Can J Cardiol. 2015;31(7):918-27. |
| 13. Perez-Carbonell L, Bashir S. Narrative review of sleep and stroke. J Thorac Dis. 2020;12(Suppl 2):S176-S90. |
| 14. Reutrakul S, Mokhlesi B. Obstructive Sleep Apnea and Diabetes: A State of the Art Review. Chest. 2017;152(5):1070-86. |
| 15. Fallahi A, Jamil DI, Karimi EB, Baghi V, Gheshlagh RG. Prevalence of obstructive sleep apnea in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab Syndr. 2019;13(4):2463-8. |
| 16. Turkay C, Ozol D, Kasapoglu B, Kirbas I, Yildirim Z, Yigitoglu R. Influence of obstructive sleep apnea on fatty liver disease: role of chronic intermittent hypoxia. Respiratory care. 2012;57(2):244-9. |
| 17. Sharafkhaneh A, Giray N, Richardson P, Young T, Hirshkowitz M. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep. 2005;28(11):1405-11. |
| 18. Leh-Kiong H CG. Signs and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance. 2020:6-12. |
| 19. Kapur VK, Auckley DH, Chowdhuri S, Kuhlmann DC, Mehra R, Ramar K, et al. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3):479-504. |
| 20. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387-94. |
| 21. Araghi MH, Chen YF, Jagielski A, Choudhury S, Banerjee D, Hussain S, et al. Effectiveness of lifestyle interventions on obstructive sleep apnea (OSA): systematic review and meta-analysis. Sleep. 2013;36(10):1553-62, 62a-62e. |
| 22. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. The Cochrane database of systematic reviews. 2006(1):Cd001106. |
| 23. Schwab RJ, Badr SM, Epstein LJ, Gay PC, Gozal D, Kohler M, et al. An official American Thoracic Society statement: continuous positive airway pressure adherence tracking systems. The optimal monitoring strategies and outcome measures in adults. American journal of respiratory and critical care medicine. 2013;188(5):613-20. |
| 24. Epstein LJ, Kristo D, Strollo PJ, Jr., Friedman N, Malhotra A, Patil SP, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2009;5(3):263-76. |
| 25. Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2019 Feb 15;15(2):335-343. |
| 26. Jacobowitz O, Afifi L, Penzel T, Poyares D, Marklund M, Kushida C; Governing Council of the World Sleep Society. Endorsement of: "treatment of adult obstructive sleep apnea with positive airway pressure: an American academy of Sleep Medicine Clinical Practice Guideline" by World Sleep Society. Sleep Med. 2022 Jan;89:19-22. |
| 27. Duong-Quy S, Nguyen-Huu H, Hoang-Chau-Bao D, Tran-Duc S, Nguyen-Thi-Hong L, Nguyen-Duy T, Tang-Thi-Thao T, Phan C, Bui-Diem K, Vu-Tran-Thien Q, Nguyen-Ngoc-Phuong T, Nguyen-Nhu V, Le-Thi-Minh H, Craig T. Personalized Medicine and Obstructive Sleep Apnea. J Pers Med. 2022 Dec 8;12(12):2034. |
| 28. BaHammam AS, Han F, Gupta R, Duong-Quy S, Al-Abri MA, Jahrami HA, Song P, Desudchit T, Xu L, Hong SB. Asian accreditation of sleep medicine physicians and technologists: practice guidelines by the Asian Society of Sleep Medicine. Sleep Med. 2021 May;81:246-252. |
ARTICLE INFO DOI: 10.12699/jfvpulm.14.44.2023.1
Conflict of Interest
Non
Date of manuscript receiving
05/09/2023
Date of publication after correction
25/10/2023
Article citation
Duong-Quy S, Nguyen-Huu H, Vu-Tran-Thien Q, Bui-Diem K, Vu-Van G, Hoang-Anh T, Nguyen-Minh S, Nguyen-Hieu H, Nguyen-Ngoc-Phuong T, Tran-Duc S, Vo-Van T, Hoang M, Nguyen-Duy T, Phan-Thanh T, Nguyen-Ngo-Hai T, Tran-Thanh-Duy L, Nguyen-Thi-Hong L, Tran-Xuan Q, Nguyen-Thi-Y N, Vo-Pham-Minh T, Tang-Thi-Thao T, Nguyen-Tuan A, Nguyen-Van T, Ngo-Duy-Tuy H, Pham-Van L, Nguyen-Xuan-Bich H, Nguyen-Hong D, Le-Thi-Minh H, Tran-Phan-Chung T, Nguyen-Nhu V, Le-Khac B. J Func Vent Pulm 2023;44(14):1-6



Copyright: jfvpulm.com