
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1611394
Visistor: 1611394Spontaneous pneumothorax revealing pulmonary metastases: A Case Study
Pneumothorax spontané révélant des métastases pulmonaires: Une étude de cas
Maryem Hindi, Sara Kechnaoui, Oussama Fikri, Lamyae Amro
Pneumology Department, Chu Mohammed VI
Labo LRMS, FMPM, UCA, Hopital Arrazi, Marrakech
Corresponding author:
Maryem HINDI
Pneumology Department, Chu Mohammed VI, Labo LRMS, FMPM, UCA, Hopital Arrazi, Marrakech
E-mail: hindi123maryem123@gmail.com
ABSTRACT
Spontaneous pneumothorax is a common pulmonary pathology. It usually occurs in patients with underlying pulmonary pathology. Spontaneous pneumothorax related to primary or metastatic malignancy is rare. The pathophysiological mechanism by which pneumothorax occurs in lung cancer is not yet well elucidated, and numerous hypotheses have been reported in the literature. Our study focuses on two cases of spontaneous pneumothorax revealing pulmonary metastases, hospitalized in the Pneumology Department of Arrazi Hospital, CHU Mohammed VI Marrakech.
KEYWORDS: Pulmonary Metastases; Spontaneous Pneumothorax; Lung Cancer.
RÉSUMÉ
Le pneumothorax spontané est une pathologie pulmonaire courante. Elle survient généralement chez des patients présentant une pathologie pulmonaire sous-jacente. Le pneumothorax spontané associé à une tumeur maligne primitive ou métastatique est rare. Le mécanisme physiopathologique par lequel le pneumothorax survient dans le cancer du poumon n'est pas encore bien élucidé et de nombreuses hypothèses ont été rapportées dans la littérature. Notre étude porte sur deux cas de pneumothorax spontané révélant des métastases pulmonaires, hospitalisés au Service de Pneumologie de l'Hôpital Arrazi, CHU Mohammed VI Marrakech.
MOTS CLÉS: Métastases pulmonaires; pneumothorax spontané; cancer du poumon.
INTRODUCTION
Spontaneous pneumothorax is a very common lung condition, usually occurring in patients with underlying pulmonary pathology such as emphysema or infectious origin (tuberculosis or ruptured hydatid cyst), but its relationship with benign or malignant, primary or metastatic tumor pathology is extremely rare, however it should be evoked in any patient with a history or risk factor of neoplastic pathology. We report two cases of spontaneous pneumothorax, revealing pulmonary metastases.
OBSERVATION
Clinical case 1.
This is a 55-year-old patient who had been treated in urology for 3 months for a tumoral process of the right kidney complicated by thrombosis of the inferior vena cava and thrombosis of the right renal vein and who was put on anticoagulant therapy (antivitamin K), who presented with right-sided stabbing chest pain
associated with Sadoul stage IV dyspnea. A chest X-ray was performed, revealing a right-sided pneumothorax of great abundance with a left interstitial syndrome (Figure 1).
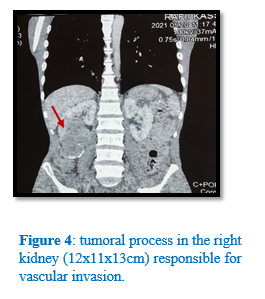
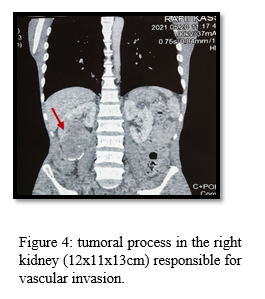
Clinical examination on admission revealed a patient with a performance status index of 4, presenting with right airway effusion syndrome. Left thoracic drainage was performed, allowing the lung to return to the wall after 6 days. On the post-drainage chest X-ray (Figure 2), we noted a diffuse bilateral interstitial syndrome with diffuse nodular opacities. A thoracic CT scan (Figure 3) revealed multiple intraparenchymal and subpleural nodules and micronodules scattered over the 2 hemi-lung fields, creating a balloon-like appearance with secondary mediastinal adenopathy. Extension work-up revealed metastatic lesions in the bone and liver, with an enormous right renal tumor process responsible for vascular invasion. The patient died two days before confirmation of the diagnosis. (Figure 4)
Clinical case 2
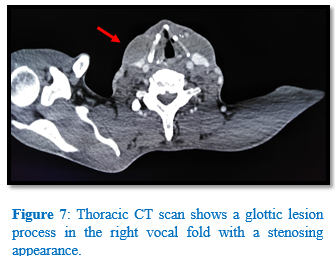
A 63-year-old patient with no specific pathological history was admitted to our clinic with abrupt onset, moderate-intensity left basithoracic stabbing pain, exacerbated by deep inspiration and coughing, associated with Sadoul stage III dyspnoea without orthopnoea, and a dry cough. A clinical examination revealed a left air pleural effusion syndrome. A chest X-ray was ordered, showing a left total pneumothorax of great abundance with deviation of mediastinal elements to the contralateral side, associated with bilateral roughly rounded intra-parenchymal opacities producing a balloon-like appearance and right apical reticulo-nodular infiltrates(Figure 5). The patient was drained, with the lung returning to the wall on the post-drainage radiograph. We completed a thoraco-abdominopelvic CT scan, revealing a glottic lesional process of the right vocal fold of stenosing appearance associated with peripheral pulmonary nodular formations of secondary appearance (Figure 6).(Figure 7).
DISCUSSION Spontaneous pneumothorax can be divided into two categories: primary and secondary. Primary SP most often affects young, healthy individuals. The secondary type may develop with obstruction, infection, infarction, neoplasm, or diffuse lung disease.
PS as a complication of lung, metastases or primary lung carcinoma is rare, with cancer found in only 0.5–3% of pneumothoraces [1, 2]. These are most often-pulmonary metastases of extra-thoracic tumors, less
frequently primary bronchial cancers, and occasionally pulmonary localizations of hematological malignancies [3]. The most common primary tumors to produce excavated metastases, and therefore PS, are those derived from epithelial tissue, genital tumors,
and sarcomas [4].
Multiple mechanisms have been proposed [5, 6] :
1/ Formation of a fistula between the parenchyma and pleura due to necrosis of a subpleural tumor nodule, secondary to vascular injury or chemotherapy.
2/ Partial bronchial obstruction by a tumor, with alveolar distension and passage of air through the alveolar spaces, then through the inter-lobular septa to the pleura, forming blebs which may rupture.
3/ Tumor embolism with infarction and necrosis.
4/ Tumor infiltration of the wall of a pre-existing benign cavity and rupture into the pleural space.
In a 1973 Mayo clinical study of 1143 patients with spontaneous pneumothorax, only ten were attributed to pulmonary malignancy, these pneumothoraxes occurred before suspicious nodules were identified on chest X-ray [9]. In the literature, a dozen cases of spontaneous pneumothorax associated with cystic images have been described; with no evidence of pulmonary metastases in the initial radiological work-up, since then, this study and the introduction of computed tomography (CT) have had their importance. In the Mayo series, all five metastatic lung tumors were sarcomas; similarly, in the cases reported by Sherman and Brant, six of the seven tumors were sarcomas and one was a metastatic adenocarcinoma.
Treatment of pneumothorax usually consists of thoracic drainage. Chemical pleurodesis is indicated to prevent recurrence. Surgery should be avoided in these patients, given the anaesthetic risk and technical difficulties involved [7,8].
CONCLUSION
Spontaneous pneumothorax secondary to tumor pathology is rarely observed. Pneumothorax may be the first sign of metastasis or lung cancer. The mechanisms by which pneumothorax occurs in lung cancer are unclear, leading to different points of view. Tumor origin should always be considered as a possible cause of PS in elderly patients or heavy smokers.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
| 1. Steinhauslin CA, Cuttat JF. Spontaneous pneumothorax. A complication of lung cancer? Chest 1985;88:709-13. |
| 2. Dines DE, Cortese DA, Bennan MD. Malignant pulmonary neoplasm predisposing to spontaneous pneumothorax. Mayo Clinic Proc 1973;48:541-4 |
| 3. Mangiapan G, Guigay J, Rosencher L, Milleron B. Le pneumothorax : une complication rare des cancers bronchiques. Rev Pneumol Clin 1992:48:284-6. |
| 4. LeGarff G, Léna H, Corbineau H, Kerbrat P, Delaval P. Unusual cause of recurrent pneumothorax: excavated metastasis of osteosarcoma. Ann Thorac Surg 2001;72:2111-3. |
| 5. Gwenaelle Le Garff, Herve Lena, Herve Corbineau, Pierre Kerbrat, and Philippe Delaval. Unusual Cause of Recurrent Pneumothorax: Excavated Metastasis of Osteosarcoma. Ann Thorac Surg 2001;72:2111–3. |
| 6. Jeffrey B. Hoag; Michael Sherman; Quadeer Fasihuddin and Mark E. Lund. A Comprehensive Review of Spontaneous Pneumothorax Complicating Sarcoma. CHEST 2010; 138(3):510–518. DOI: 10.1378/chest.09- |
| 7. Mezghani S, Benzarti M, Njima H, Hayouni A, Garrouche A, Klabi N, et al. Un pneumothorax spontané récidivant compliquant les metastases pulmonaires d’un ostéosarcome. Rev Pneumol Clin 2005;61:50—2. |
| 8. Rammohan G, Bonacini M, Dwek JH, Das A. Pleurodesis in metastatic pneumothorax. Chest 1986;90:918—9. |
| 9. Dines DE, Cortese DA, Brennan MD, Hahn RG, Payne WS. Malignant pulmonary neoplasms predisposing to spontaneous pneumothorax. Mayo Clin Proc 1973;48:541—4. |

Figures





REFERENCES
| 1. Steinhauslin CA, Cuttat JF. Spontaneous pneumothorax. A complication of lung cancer? Chest 1985;88:709-13. |
| 2. Dines DE, Cortese DA, Bennan MD. Malignant pulmonary neoplasm predisposing to spontaneous pneumothorax. Mayo Clinic Proc 1973;48:541-4 |
| 3. Mangiapan G, Guigay J, Rosencher L, Milleron B. Le pneumothorax : une complication rare des cancers bronchiques. Rev Pneumol Clin 1992:48:284-6. |
| 4. LeGarff G, Léna H, Corbineau H, Kerbrat P, Delaval P. Unusual cause of recurrent pneumothorax: excavated metastasis of osteosarcoma. Ann Thorac Surg 2001;72:2111-3. |
| 5. Gwenaelle Le Garff, Herve Lena, Herve Corbineau, Pierre Kerbrat, and Philippe Delaval. Unusual Cause of Recurrent Pneumothorax: Excavated Metastasis of Osteosarcoma. Ann Thorac Surg 2001;72:2111–3. |
| 6. Jeffrey B. Hoag; Michael Sherman; Quadeer Fasihuddin and Mark E. Lund. A Comprehensive Review of Spontaneous Pneumothorax Complicating Sarcoma. CHEST 2010; 138(3):510–518. DOI: 10.1378/chest.09- |
| 7. Mezghani S, Benzarti M, Njima H, Hayouni A, Garrouche A, Klabi N, et al. Un pneumothorax spontané récidivant compliquant les metastases pulmonaires d’un ostéosarcome. Rev Pneumol Clin 2005;61:50—2. |
| 8. Rammohan G, Bonacini M, Dwek JH, Das A. Pleurodesis in metastatic pneumothorax. Chest 1986;90:918—9. |
| 9. Dines DE, Cortese DA, Brennan MD, Hahn RG, Payne WS. Malignant pulmonary neoplasms predisposing to spontaneous pneumothorax. Mayo Clin Proc 1973;48:541—4. |
ARTICLE INFO DOI: 10.12699/jfvpulm.14.44.2023.40
Conflict of Interest
Non
Date of manuscript receiving
25/04/2023
Date of publication after correction
25/10/2023
Article citation
Maryem Hindi, Sara Kechnaoui, Oussama Fikri, Lamyae Amro. J Func Vent Pulm 2023;44(14):40-43



Copyright: jfvpulm.com
{kind=link}