
 English
English
 French
French
 Pubmed
Pubmed Google Scholar
Google Scholar Cross Ref
Cross Ref Visistor: 1775629
Visistor: 1775629Late diagnosis of pulmonary agenesis in a 58 years-old woman
Diagnostic tardif d’une agénésie pulmonaire chez une femme de 58 ans
M. Zoutené1, A.M.E. Ako1, B. Mewezinoh1, B. Bilivogui 1, K.S. Adjoh1,2
1Department of Pulmonology, Sylvanus Olympio University Hospital, Lomé, Togo.
2Faculty of Health Sciences, University of Lomé, Lomé, Togo.
Corresponding author: Maissala Zoutene. Department of Pulmonology, Sylvanus Olympio University Hospital, Lomé, Togo.
Email: zoutenemaissala@gmail.com .
ABSTRACT
Introduction. Pulmonary agenesis is a rare congenital anomaly associated with a poor prognosis due to the frequent presence of multiple associated malformations. Asymptomatic cases with delayed diagnosis in adulthood are uncommon.
Case presentation. We report a case of isolated pulmonary agenesis incidentally revealed by the onset of asthma in a 58-year-old woman with no prior respiratory history. Her medical history included a myomectomy in 2014. She was referred to the Department of Pulmonology at Sylvanus Olympio University Teaching Hospital for dyspnea associated with a unilateral left “white lung” appearance on chest radiography. The dyspnea had been evolving for four weeks, characterized by recurrent episodes with progressive worsening. Physical examination revealed tachypnea at 26 breaths per minute, peripheral oxygen saturation of 94% on room air, asymmetry of the left hemithorax with signs of retraction, and absent breath sounds. Chest radiography demonstrated a homogeneous water-density opacity occupying the entire left lung field with mediastinal shift towards the left side. . An abrupt termination of the left pulmonary artery, along with cardiac deviation and rotation, was also noted in Chest-CT scan.
Conclusion. Late-diagnosed pulmonary agenesis is not exceptional and is frequently associated with an obstructive ventilatory disorder.
KEYWORDS: Pulmonary agenesis; Unilateral; Asthma; Adult.
RÉSUMÉ
Introduction. L’agénésie pulmonaire est une anomalie congénitale rare, associée à un pronostic défavorable en raison de la présence fréquente de multiples malformations associées. Les formes asymptomatiques avec diagnostic tardif à l’âge adulte sont peu fréquentes.
Présentation du cas. Nous rapportons un cas d’agénésie pulmonaire isolée, découverte fortuitement à l’occasion de l’apparition d’un asthme chez une femme de 58 ans sans antécédents respiratoires. Ses antécédents médicaux comprenaient une myomectomie en 2014. Elle a été adressée au service de pneumologie du Centre Hospitalier Universitaire Sylvanus Olympio pour une dyspnée associée à un aspect de « poumon blanc » unilatéral gauche à la radiographie thoracique.La dyspnée évoluait depuis quatre semaines, caractérisée par des épisodes récurrents avec une aggravation progressive. L’examen clinique retrouvait une tachypnée à 26 cycles par minute, une saturation périphérique en oxygène à 94 % à l’air ambiant, une asymétrie de l’hémithorax gauche avec des signes de rétraction, ainsi qu’une abolition du murmure vésiculaire. La radiographie thoracique montrait une opacité homogène de tonalité hydrique occupant tout le champ pulmonaire gauche, avec une déviation médiastinale vers le côté gauche. Une interruption brutale de l’artère pulmonaire gauche, associée à une déviation et une rotation cardiaques, était également notée au scanner thoracique.
Conclusion. L’agénésie pulmonaire diagnostiquée tardivement n’est pas exceptionnelle et s’accompagne fréquemment d’un trouble ventilatoire obstructif.
MOTS CLÉS: Agénésie pulmonaire; Unilatérale; Asthme; Adulte.
INTRODUCTION
Congenital pulmonary malformations are rare conditions that occur early during intra-uterine development [1]. Pulmonary agenesis refers to the partial or complete absence of pulmonary growth [2]. In most cases, the diagnosis is established at birth or during childhood; however, asymptomatic forms with delayed presentation in adulthood do occur. We report here a case diagnosed in the Department of Pulmonology at Sylvanus Olympio University Teaching Hospital in Lomé, Togo.
CASE PRESENTATION
A 58-year-old woman, mother of three children all born by uncomplicated vaginal delivery, was followed for arterial hypertension treated with an indapamide/amlodipine combination. Her medical history included a myomectomy in 2014. She was referred to the Department of Pulmonology at Sylvanus Olympio University Teaching Hospital for dyspnea associated with a unilateral left “white lung” appearance on chest radiography.
The dyspnea had been evolving for four weeks, characterized by recurrent episodes with progressive worsening. Physical examination revealed tachypnea at 26 breaths per minute, peripheral oxygen saturation of 94% on room air, asymmetry of the left hemithorax with signs of retraction, and absent breath sounds. Chest radiography demonstrated a homogeneous water-density opacity occupying the entire left lung field with mediastinal shift towards the left side (Figure 1). Electrocardiography showed regular sinus tachycardia at 111 beats per minute.
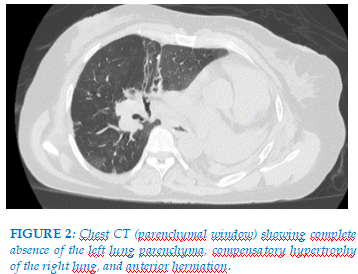
Lung ultrasound revealed no pleuro-pulmonary line and no pleural effusion, but cardiac chambers were visualized. Chest computed tomography demonstrated complete absence of left pulmonary parenchyma with compensatory hypertrophy of the right lung (Figure 2).
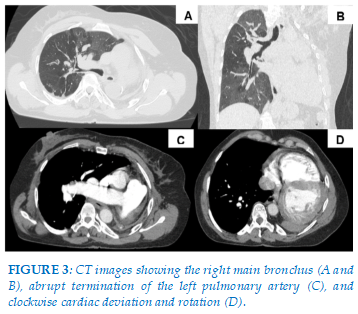
An abrupt termination of the left pulmonary artery, along with cardiac deviation and rotation, was also noted (Figure 3). Flexible bronchoscopy showed that immediately beyond the trachea, the airway continued directly into the right main bronchus. Histopathological examination of a biopsy from the bronchial spur between the upper and middle lobar bronchi, as well as cytological analysis of bronchoalveolar lavage, revealed no evidence of malignancy or infection. A diagnosis of pulmonary agenesis was established. Spirometry demonstrated a forced vital capacity (FVC) of 0.94 L (44% predicted), an FEV1/FVC ratio of 56.4% (82% predicted), and a pre-bronchodilator forced expiratory volume in one second (FEV1) of 530 mL (31% predicted). Post-bronchodilator FEV1, measured 15 minutes after four puffs of 100 μg salbutamol, increased to 750 mL (44% predicted). These findings indicated airflow obstruction with a post-bronchodilator FEV1 improvement of 220 mL (13%), and a probable associated restrictive ventilatory defect. Cardiac and abdominal ultrasound examinations did not reveal any associated malformations. Treatment with a combination of formoterol 6 μg and budesonide 200 μg was initiated.
DISCUSSION
Pulmonary developmental defects are classified into three distinct groups [3]. Group I, also called pulmonary agenesis is characterized by the complete absence of unilateral lung parenchyma, bronchus, and vasculature. In group II, namely pulmonary aplasia, there is a complete absence of unilateral lung with a rudimentary blind-ending bronchus. In group III, pulmonary hypoplasia, there is bronchial hypoplasia with a variable amount of remaining lung tissue. The case of our patient corresponds to the characteristics of Group I.
The exact etiology of pulmonary agenesis remains unknown, but its pathophysiology is thought to involve interactions among genetic, environmental, and mechanical factors [4,5]. The condition is often diagnosed early in life, with nearly half of affected individuals dying within the first five years; however, rare asymptomatic cases with delayed diagnosis in adulthood have been reported [6,7]. The oldest reported patient was 72 years old [8]. Our patient, aged 58 years, therefore falls into the category of late diagnoses. Her favorable prognosis is consistent with pre vious reports in the literature. In our case, the anomaly involved the left lung, and no associated malformations of other organs were identified. Indeed, right-sided pulmonary agenesis, which is more frequently associated with additional malformations, tends to have a poorer prognosis compared with left-sided agenesis [9]. The reversible obstructive ventilatory defect observed in our patient corroborates the findings of Kushwaha et al. [1] in India and those of Pimenta et al. [10] in Portugal. Kushwaha’s patient had a family history of asthma, whereas our patient had no personal or family history of asthma. There is no specific treatment for pulmonary agenesis; management is primarily symptomatic, combined with regular follow-up. Surgical intervention may be considered on a case-by-case basis [11].
CONCLUSION
Pulmonary agenesis with delayed diagnosis is not uncommon and appears to occur predominantly in cases of left lung agenesis. Prognosis depends on the extent of the anomalies and on the presence or absence of associated malformations.
REFERENCES
| 1. Part RAS, Ranganath TG, Garg R, Anand S. Complete right lung agenesis presenting with bronchial asthma and allergic rhinitis. Case Rep. 2012;2012:bcr0120125553. |
| 2. Roy PP, Datta S, Sarkar A, Das A, Das S. Unilateral pulmonary agenesis presenting in adulthood. Respir Med Case Rep. 2012;5:81–3. https://doi.org/10.1016/j.rmedc.2011.05.003. |
| 3. Alwan A, Mohammoud S, Assefa AZ. Incidental pulmonary agenesis with multiple associated anomalies: A case report. Radiol Case Rep. 2023;18:3724–3728. |
| 4. Berrocal T, Madrid C, Novo S, Gutiérrez J, Arjonilla A, Gómez-León N. Congenital Anomalies of the Tracheobronchial Tree, Lung, and Mediastinum: Embryology, Radiology, and Pathology. RadioGraphics. 2004;24:e17–e17. https://doi.org/10.1148/rg.e17. |
| 5. Kaya O, Gulek B, Yilmaz C, Soker G, Esen K, Akin MA, et al. Adult presentation of symptomatic left lung agenesis. Radiol Case Rep. 2017;12:25. |
| 6. Ta RK, Banerjee SN, Chatterjee K. Agenesis of left lung in an adult female: a rare case report. Muller J Med Sci Res. 2015;6:172–174. |
| 7. Komolafe F, Dahniya MH, Al-Ali Y, Al-Zaabi L, Aziz F. Asymptomatic unilateral pulmonary hypoplasia/agenesis in adults: a report of six cases. West Afr J Radiol. 2017;24:99–103. |
| 8. Black PR, Welch KJ. Pulmonary agenesis (Aplasia), esophageal atresia, and Tracheoesophageal fistula: A different treatment strategy. J Pediatr Surg. 1986;21:936–8. https://doi.org/10.1016/S0022-3468(86)80094-X. |
| 9. Kumar P, Tansir G, Sasmal G, Dixit J, Sahoo R. Left pulmonary agenesis with right lung bronchiectasis in an adult. J Clin Diagn Res JCDR. 2016;10:OD15. |
| 10. Pimenta DA, Aguiar FL, Fernandes BC, Rolo R. Late diagnosis of pulmonary agenesis. BMJ Case Rep CP. 2021;14:e245233. |
| 11. Krivchenya DU, Rudenko EO, Lysak SV, Dubrovin AG, Khursin VN, Krivchenya TD. Lung Aplasia: Anatomy, History, Diagnosis and Surgical Management. Eur J Pediatr Surg. 2007;17:244–50. https://doi.org/10.1055/s-2007-965200. |

FIGURES - TABLES

REFERENCES
| 1. Part RAS, Ranganath TG, Garg R, Anand S. Complete right lung agenesis presenting with bronchial asthma and allergic rhinitis. Case Rep. 2012;2012:bcr0120125553. |
| 2. Roy PP, Datta S, Sarkar A, Das A, Das S. Unilateral pulmonary agenesis presenting in adulthood. Respir Med Case Rep. 2012;5:81–3. https://doi.org/10.1016/j.rmedc.2011.05.003. |
| 3. Alwan A, Mohammoud S, Assefa AZ. Incidental pulmonary agenesis with multiple associated anomalies: A case report. Radiol Case Rep. 2023;18:3724–3728. |
| 4. Berrocal T, Madrid C, Novo S, Gutiérrez J, Arjonilla A, Gómez-León N. Congenital Anomalies of the Tracheobronchial Tree, Lung, and Mediastinum: Embryology, Radiology, and Pathology. RadioGraphics. 2004;24:e17–e17. https://doi.org/10.1148/rg.e17. |
| 5. Kaya O, Gulek B, Yilmaz C, Soker G, Esen K, Akin MA, et al. Adult presentation of symptomatic left lung agenesis. Radiol Case Rep. 2017;12:25. |
| 6. Ta RK, Banerjee SN, Chatterjee K. Agenesis of left lung in an adult female: a rare case report. Muller J Med Sci Res. 2015;6:172–174. |
| 7. Komolafe F, Dahniya MH, Al-Ali Y, Al-Zaabi L, Aziz F. Asymptomatic unilateral pulmonary hypoplasia/agenesis in adults: a report of six cases. West Afr J Radiol. 2017;24:99–103. |
| 8. Black PR, Welch KJ. Pulmonary agenesis (Aplasia), esophageal atresia, and Tracheoesophageal fistula: A different treatment strategy. J Pediatr Surg. 1986;21:936–8. https://doi.org/10.1016/S0022-3468(86)80094-X. |
| 9. Kumar P, Tansir G, Sasmal G, Dixit J, Sahoo R. Left pulmonary agenesis with right lung bronchiectasis in an adult. J Clin Diagn Res JCDR. 2016;10:OD15. |
| 10. Pimenta DA, Aguiar FL, Fernandes BC, Rolo R. Late diagnosis of pulmonary agenesis. BMJ Case Rep CP. 2021;14:e245233. |
| 11. Krivchenya DU, Rudenko EO, Lysak SV, Dubrovin AG, Khursin VN, Krivchenya TD. Lung Aplasia: Anatomy, History, Diagnosis and Surgical Management. Eur J Pediatr Surg. 2007;17:244–50. https://doi.org/10.1055/s-2007-965200. |
ARTICLE INFO DOI:10.12699/jfvpulm.17.51.2026.76
Conflict of Interest
Non
Date of manuscript receiving
10/9/2025
Date of publication after correction
9/12/2025
Article citation
M.Zoutené, A.M.E. Ako, B. Mewezinoh, B. Bilivogui, K.S. Adjoh. Late diagnosis of pulmonary agenesis in a 58 years-old woman. J Fran Vent PulmS 2026;51(17):77-79



Copyright: jfvpulm.com